 by Murali K. Kolikonda, MD; Suneela Cherlopalle, MD; Manasa Enja, MD; and Steven Lippmann, MD
by Murali K. Kolikonda, MD; Suneela Cherlopalle, MD; Manasa Enja, MD; and Steven Lippmann, MD
Drs. Kolikonda, Cherlopalle, Enja, and Lippmann are with the University of Louisville School of Medicine, Department of Psychiatry, Louisville, Kentucky.
Innov Clin Neurosci. 2015;12(3–4):24–26.
Funding: There was no funding for the development and writing of this article.
Financial disclosures: The authors have no affiliations with or financial interest in any organization that may pose any conflict of interest.
Key words: pentazocine, analgesia, myopathy, intramuscular pentazocine, drug-induced myopathy, pentazocine-induced muscular side-effect, pentazocine-induced muscular adversity
Abstract: Pentazocine is a mixed agonist/antagonist opioid analgesic agent that can induce an atypical myopathy following intramuscular injections. This iatrogenic myopathy is rare, typified by fibrosis, and should be differentiated from other myopathies. We describe a case of pentazocine-induced myopathy that caused wasting of musculature in the gluteal region bilaterally and stiffness and woody induration in the legs of 42-year-old man. Though rare, clinicians should be alerted to this potential side effect and avoid repeated administration of intramuscular pentazocine.
Introduction
Pentazocine is a synthetic opioid commonly prescribed for analgesia in developing countries. It is a schedule IV drug in the United States and a schedule III pharmaceutical under the Convention on Psychotropic Substances for developing countries. Upon intramuscular injection, it can induce an iatrogenic myopathy as one of its numerous side effects. With adversities similar to morphine and with actions on the kappa opioid receptor, it may induce a psychosis.[1] Substance abuse is another concern about pentazocine that requires close monitoring. Pentazocine, especially in its intramuscular form, is rarely used in most medically advanced countries, but is still sometimes prescribed in areas that are less medically advantaged. Clinicians should be alerted to the potential of an atypical myopathy following intramuscular injections, and avoid repeated administration of intramuscular pentazocine in their patients.
Clinical Vignette
A 42-year-old man presented with painless, progressive, and persistent stiffness of the legs for eight months. The patient complained about impairment in walking, bending, and rising from a supine or squatting position. He also noted loss of muscle power and mass in the gluteal region over the last year.
Because of chronic epigastric pain, the patient had been receiving pentazocine injections in the gluteal musculature. The history revealed that he had been administered 60mg intramuscular pentazocine daily for 1.5 years.
The cranial examination was normal. Wasting of musculature at the gluteal region bilaterally was evident, as depicted in Figure 1, along with woody induration of the lower limbs, as seen in Figure 2. Range of motion was restricted; legs could not be abducted more than 30°. Unable to cross his legs, hip flexion was limited to 10 degrees. Muscle power in the arms was normal bilaterally, but weak in both lower extremities. Deep tendon reflexes could not be elicited in the legs, and plantar response was flexor bilaterally. Sensory, autonomic, and cerebellar functions were intact.


Laboratory studies included a normal hemogram, chemistry profile, calcium, phosphorus, and parathormone. The creatinine phosphokinase was elevated and at 367 IU/L (the normal range is between 8–150 IU/L). X-ray imaging of the lumbosacral spine and knees were unremarkable. Electroneuromyography was physiologic in the upper limbs, but in the lower extremities revealed bilaterally reduced compound muscle action potentials in the peroneal and posterior tibial nerves. Sural sensory nerve action potentials were bilaterally absent.
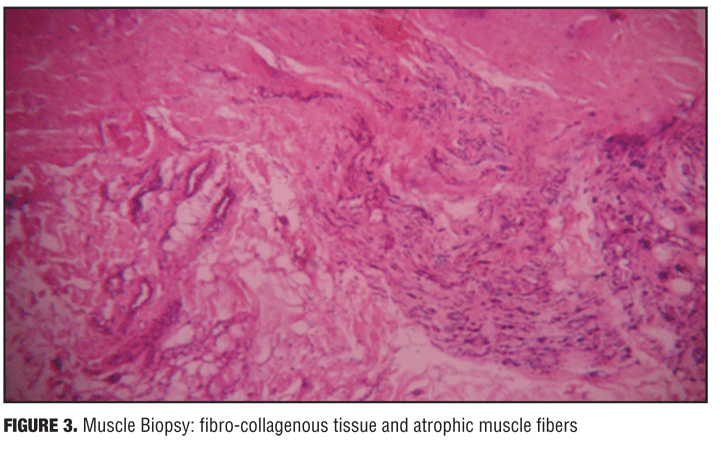
Pentazocine-induced myopathy was the clinical diagnosis by history and physical examination. A gluteal muscle biopsy revealed myofibrosis, as noted in Figure 3, and confirmed this impression.
Discussion
Pentazocine is a synthetic analgesic medication prescribed for the relief of pain. It is often utilized parenterally; however, a fibrous myopathy is a rare, but significant complication following intramuscular pentazocine injections.[2] Cutaneous adversities include fibrosis, brawny induration, ulceration, and abnormal skin pigmentation, which can also follow parenteral usage.
The exact mechanism of action is unclear. Precipitation of the drug in the muscle, pharmaceutical presence there or in the vein, or an independent factor released at the site of injection is proposed etiologically. The pentazocine precipitates in muscle along with the trauma caused by the repeated injection of large quantity drug boluses may be the cause of this localized myopathy.[3] The frequent administration of 60 to 240mg doses can produce these complications.
Further muscle damage can be prevented, if intramuscular injections are discontinued. Physical therapy may facilitate functional improvement in mild cases. When muscle fibrosis is extensive, surgical section of fibrous bands and disinterment of muscle tendon might offer some relief. Cutaneous ulcers are managed by excision and skin grafting.
Table 1 lists differential diagnoses for atypical myopathy. Table 2 lists side effects of pentazocine.[4–9]
Conclusion
Pentazocine-induced myopathy is a rare complication in patients repeatedly prescribed intramuscular pentazocine injections. Consider it in the differential diagnosis of any myopathy with fibrosis and rule-out polymyositis or other myopathies. Affected muscle groups should be evaluated by electromyography and/or biopsy. In all cases, rotate injection sites if repetitive therapy is necessary and avoid intramuscular pentazocine as much as possible.
References
1. Goyal V, Chawla JM, Balhara YP, et al. Calcific myofibrosis due to pentazocine abuse. J Med Case Rep. 2008;2:160.
2. Adams EM, Horowitz HW, Sundstrom WR. Fibrous myopathy in association with pentazocine. Arch Intern Med. 1983;143:2203–2204.
3. Das C, Thussu A, Prabhakar S, Banerjee A. Pentazocine-induced fibromyositis and contracture. Postgrad Med J. 1999;75:361–363.
4. Sinsawaiwong S, Phanthumchinda K. Pentazocine-induced fibrous myopathy and localized neuropathy. J Med Assoc Thai. 1998;81:717–721.
5. Fleming JD, Hopper A, Robson A, et al. Pentazocine-induced cutaneous scarring. Clin Exp Dermatol. 2014;39:115–116.
6. Kathuria S, Ramesh V, Singh A. Pentazocine induced ulceration of the buttocks. Indian J Dermatol Venereol Leprol. 2012;78:521.
7. Rousseau JJ, Reznik M, LeJeune GN, Franck G. Sciatic nerve entrapment by pentazocine-induced muscle fibrosis: a case report. Arch Neurol. 1979;36:723–724.
8. Riley JL, Hastie BA, Glover TL, et al. Cognitive-affective and somatic side effects of morphine and pentazocine: side-effect profiles in healthy adults. Pain Med. 2010;11:195–206.
9. Mudrick C, Isaacs J, Frankenhoff J. Injectable pentazocine abuse leading to necrotizing soft tissue infection and florid osteomyelitis. HAND. 2011;6:457–459.




{kind=link}
{kind=link}
{kind=link}
{kind=link}