
 by Emily Leppien, PharmD, BCPS; Kimberly Mulcahy, PharmD, BCPS, BCPP; Tammie Lee Demler, BS, PharmD, MBA, BCGP, BCPP; Eileen Trigoboff, RN, PMHCNS-BC, DNS, DABFN; and Lewis Opler, MD, PhD†
by Emily Leppien, PharmD, BCPS; Kimberly Mulcahy, PharmD, BCPS, BCPP; Tammie Lee Demler, BS, PharmD, MBA, BCGP, BCPP; Eileen Trigoboff, RN, PMHCNS-BC, DNS, DABFN; and Lewis Opler, MD, PhD†
Drs. Leppien, Mulcahy, Demler, and Trigoboff are with Buffalo Psychiatric Center, New York State Office of Mental Health, and State University of New York, University at Buffalo School of Pharmacy and Pharmaceutical Sciences in Buffalo, New York. Drs. Demler and Trigoboff are with State University of New York, University at Buffalo School of Medicine, Department of Psychiatry. in Buffalo, New York. Dr. Opler is affiliated with Long Island University in Long Island, New York. †deceased
Innov Clin Neurosci. 2018;15(3–4):24–27
Funding: None
Disclosures: The authors declare no conflicts of interest relevant to the content of this article.
Abstract: Overview. Psychiatric adverse effects, including aggression, have been reported with the use of statin medications; however, there is little data to support or refute the theory that statins or low serum cholesterol do in fact increase a patient’s risk of aggression.
Objective. This study examined 1) statin use and increased aggression, measured by the requirement of either emergent psychiatric intervention referred to as “Code Green” (CG) or “Restraint and Seclusion” (RS) and 2) cholesterol level and increased aggression in psychiatric inpatients.
Materials and Methods. Patient charts from January 1, 2011, to December 31, 2015 were reviewed. Statin therapy, lipid panel, and requirement of a psychiatric emergency code CG or RS were noted. Inpatients who did not receive cholesterol-lowering therapy were used as controls. Analyses of variance (ANOVAs) were used to examine the relationship between statin use and increased aggression.
Results. Eleven (9.6%) patients receiving statins required a total of 57 CGs, and five (4.4%) required 27 RSs. Conversely, 33 (28.9%) patients not receiving statins required a total of 64 CGs, and 14 (12.3%) required 27 RSs. No statistically significant relationship between statin therapy and agitation was found as evidenced by a CG (F=0.068; p=0.795) or RS (F=0.001; p=1.000). A statistically significant relationship was found between total cholesterol level and requirement of a CG (F=1.435; p=0.029) or RS (F=2.89; p=0.000).
Conclusion. It is evident that psychiatric inpatients with lower total cholesterol levels are at an increased risk for loss of behavioral control.
Keywords: Statins, cholesterol, aggression, agitation, violence, psychiatric inpatients
Little data support or refute the claim that statins or low serum cholesterol increase a patient’s risk of aggression. Therefore, it is imperative that we, as healthcare professionals, contribute to best practices to ensure that we do not inadvertently worsen a patient’s preexisting psychiatric condition. Behavioral changes can be provoked by a variety of medications. Recent literature has linked 3-hydroxy-3-methyl-glutaryl-coenzyme A (HMG-CoA) reductase inhibitors, commonly referred to as statins, to central nervous system (CNS) neuropsychiatric adverse effects, including aggression, agitation, irritability, mood changes, violent ideation, sleep problems, suicidality, and additional behavioral disturbances.1–5 These adverse effects have also been reported in the setting of low cholesterol and with lower omega-3 fatty acid levels.6–9
Several mechanisms have been proposed to explain the association between lowered cholesterol and behavioral changes. Lipids play an important role in brain functioning and are critical in the formation of neuron cell membranes, myelin sheath, and nerve synapses. It has been hypothesized that decreased serum lipid levels in the brain can reduce obtainable cholesterol by neurons, which can lower serotonergic activity by decreasing serotonin receptor expression. Serotonin plays a vital role in behavioral control, and alterations to the serotonergic pathway or serotonin availability can result in changes in behavioral control and psychiatric adverse effects.3
Connections between mitochondrial dysfunction and psychiatric adverse effects have been previously documented. Statins might lead to mitochondrial dysfunction and oxidative stress; while the precise mechanism is unknown, there is evidence that statins lead to depletion of coenzyme Q10 (CoQ10), a mitochondrial nutrient needed to transport fatty acids to and within the mitochondria. During cholesterol synthesis, various metabolites, including CoQ10, are produced. Plasma levels of CoQ10 would therefore be lowered during treatment with HMG-CoA reductase inhibitors. It has also been documented that lower CoQ10 plasma levels could possibly be a result of decreased low-density lipoprotein (LDL), as CoQ10 is mainly transported by LDL.10
Statins might secondarily cause behavioral changes through their impact on a variety of different factors, including impaired sleep, reduced testosterone, and effects on oxidative stress. Impaired or decreased sleep has been linked to irritability, aggression, and violence. However, behavioral changes associated with statin therapy might also be protective, as lower testosterone levels have been linked to reduced aggressive behavior.1
In a 2015 case series, Cham et al1 found that cholesterol-lowering therapy was associated with behavioral changes, including aggression, mood or personality changes, and violent or homicidal/suicidal ideation. These psychiatric adverse effects resolved upon drug discontinuation and recurred upon rechallenge, which suggests a causative relationship. The behavioral changes observed all had negative implications for marriages, careers, and/or safety of self and others. As a potential confounder, it should be noted that some of the patients in this series had underlying psychiatric conditions, indicating that psychiatric illnesses might be worsened.1 Sahebzamani et al5 reported conflicting relationships between cholesterol levels (specifically LDL and total cholesterol) and self-reported ratings of depression, aggression, cynicism, and hostility. Reduced LDL (<100mg/dL) was associated with increased hostility in a subgroup of Caucasian patients receiving cholesterol-lowering therapy and significantly greater aggression scores in patients concomitantly prescribed psychiatric medication. However, after adjustment for factors that can influence aggressive behaviors, a low LDL was not independently associated with aggression.5
Golomb et al11 reported that post-menopausal women over 45 years of age, with lower levels of aggression at baseline, who were treated with either simvastatin 20mg or pravastatin 40mg exhibited significantly increased aggressive behaviors compared to those treated with placebo after the six-month trial period. Conversely, male patients 40 years of age or younger, with higher levels of aggression at baseline, showed decreased aggressive behaviors compared to those treated with placebo. However, this significance was only observed after the removal of three marked male outliers. Otherwise, statin use did not result in a significant change in aggression from baseline.11
Recent studies examining the association between statin therapy and increased aggressive behavior have shown conflicting results, which has further complicated the possible relationship between cholesterol-lowering therapy and increased occurrence of loss of behavioral control. The cardiovascular benefits associated with statins are well-documented, and because patients with serious mental illness (SMI) experience a disproportionate degree of early mortality associated with cardiovascular complications when compared to their non-SMI peers, a relationship between their use and aggression might negatively influence how hypercholesterolemia and atherosclerotic cardiovascular disease (ASCVD) risk reduction is managed in this population.12 Our study evaluates whether the use of statin therapy or low cholesterol levels increase the incidence of aggression and behavioral changes in a psychiatric inpatient population.
Objectives
There were two hypotheses tested in this study. The primary hypothesis was to determine whether statin use increased the risk of aggression and agitation, while the second hypothesis was to determine if low serum cholesterol level increased the risk of aggression in adult psychiatric patients admitted for inpatient hospitalization at a state psychiatric facility.
Methods
The study was approved by the Institutional Review Board of record for the facility (New York State Psychiatric Institute). A retrospective patient chart review of adult inpatients who were hospitalized at a state psychiatric center between January 1, 2011, and December 31, 2015, was conducted. For the first hypothesis, patient charts were evaluated for the receipt of statin therapy and the date statin therapy was initiated. For the second hypothesis, patient charts were evaluated for fasting lipid panels, specifically total cholesterol, within one year of starting statin therapy or within one year of admission. For both hypotheses, agitation and aggression were measured by the requirement of an emergent psychiatric intervention “code green” (CG) or the intervention of a restraint or seclusion (RS) within one year of starting statin therapy or within one year of admission.
There were 114 patients on statin therapy who met all inclusion criteria for both hypotheses. Of the 144 patients who met all inclusion criteria and did not receive statin therapy during their admission, 114 patients were randomly selected to serve as matched controls. Analysis of variance (ANOVA) statistical analyses were conducted using the Statistical Package for Social Sciences version 23 (SPSS v23) to evaluate the risk of increased aggression relative to statin use or as a consequence of low serum total cholesterol levels. The level for statistical significance was selected at p<0.05 to minimize the risk of Type I error.
To be included in the study for either hypothesis, patients had to be older than 18 years of age and be inpatients at the state psychiatric center any time between January 1, 2011, and December 31, 2015. Patients admitted prior to January 1, 2011, or those who had a Criminal Procedure Law (CPL) designation were excluded. For the first hypothesis, patients with unknown statin therapy status or those initiated on statin therapy for more than 30 days following admission were excluded. To be included in the study for the second hypothesis, patients were required to have had a lipid panel obtained during the first year of admission or within one year of starting statin therapy.
Results
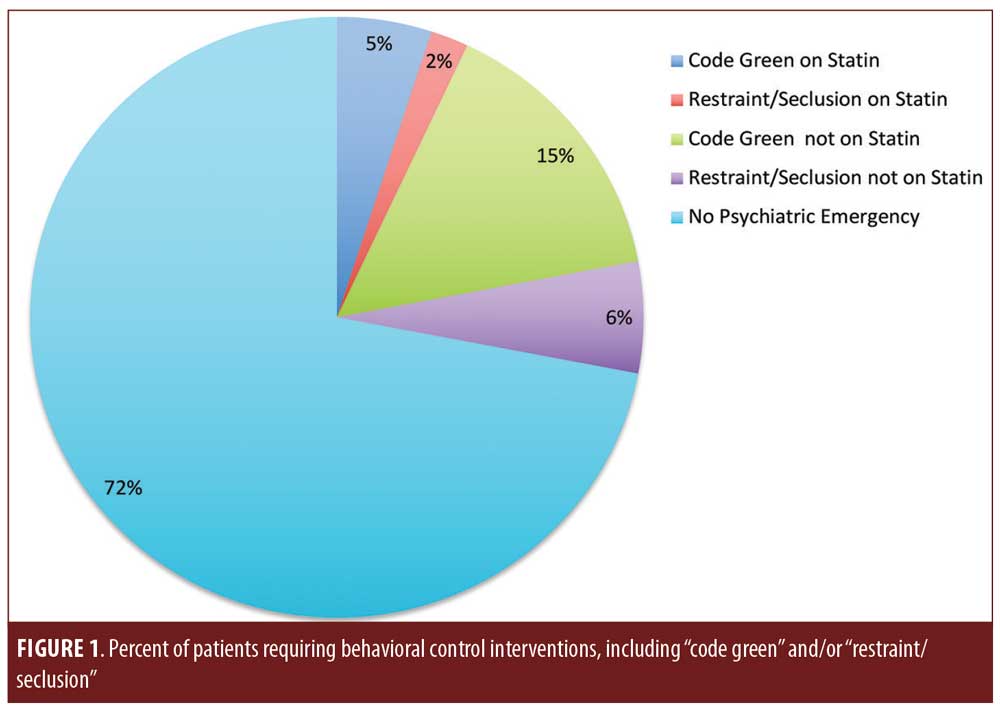
Charts of 754 patients were reviewed. ANOVA testing was used to evaluate whether an increased risk of aggression and loss of behavioral control was observed in patients receiving statin therapy or with low serum cholesterol levels. Cholesterol levels were categorized into low, low normal, normal, and high levels. Of the 96 patients with low TCL, 50 were on a statin and 46 were not. Of the 69 patients with low normal TCL, 32 were on a statin and 37 were not. Of the 42 patients with normal TCL, 18 were on a statin and 24 were not. And of the 22 patients with high TCL, 15 were on a statin and seven were not. A total of 228 patients were included in the analysis. Eleven patients who were receiving statin therapy required at least one CG (5%), while five patients who were receiving statin therapy required at least one RS (2%). Thirty-three patients who were not receiving statin therapy required at least one CG (15%), while 14 patients who were not receiving statin therapy required at least one RS (6%). The remaining 165 patients (72%) included in the analysis did not require an emergent psychiatric intervention (Figure 1).
Of the 114 patients on statin therapy, 11 (9.6%) required a total of 57 CGs and five (4.4%) required 27 RSs within one year of starting statin therapy. Of the 114 patients not receiving statin therapy, 33 (28.9%) required a total of 64 CGs and 14 (12.3%) required 27 RSs during their first year of inpatient hospitalization. Using ANOVA, we found no statistically significant relationship between statin therapy and loss of behavioral control as evidenced by a CG (F=0.068; p=0.795) or use of RS (F=0.000; p=1.000).
The mean total cholesterol levels were similar between the two groups (176.5mg/dL for those receiving statin therapy and
174.8mg/dL for those not receiving statin therapy), which facilitated the analysis of total serum cholesterol level versus CG and RS. Using ANOVA to assess the full range of cholesterol levels collected, a statistically significant relationship was found between total cholesterol level and requirement of a CG (F=1.435; p=0.029) and RS (F=2.891; p=0.000), indicating that increased psychiatric emergencies appear to be associated with total cholesterol level. Patients with lower total serum cholesterol levels in this inpatient sample were more likely to experience aggression and loss of behavioral control than those with normal or elevated serum cholesterol levels.
Discussion
We found no statistical significance in the proposed relationship between receiving statin therapy and an increased incidence of CG or RS. Therefore, our results do not replicate the findings reported in the current literature supporting the hypothesis that the use of statin therapy results in an increased risk of patient aggression. The majority of our patients on statin therapy were either admitted to our psychiatric facility having already been prescribed statin therapy or had statin therapy initiated by an inpatient provider within 30 days of their admission. If the patient was initiated on statin therapy prior to hospital admission, the duration of his or her therapy prior to becoming an inpatient was unknown. Aggression, agitation, or loss of behavioral control could also have been measured by the number of psychiatric PRNs given; unfortunately, we were unable to effectively compare any differences in PRN medication use because all 114 patients were either admitted to the hospital receiving statin therapy or were initiated on statin therapy within 30 days of admission, which would not provide an adequate time period for comparison. Future analysis could be beneficial in examining this possible relationship, as PRN medications are often administered as a de-escalation intervention prior to the requirement of a CG/RS.
We were unable to analyze whether different statin medications could have contributed to increased aggression in the psychiatric inpatient population as many patients changed statin therapy throughout their hospitalization due to insurance formulary changes, and there was not a robust nor equal number of patients receiving each particular statin. Due to the small sample size, we were also unable to conduct a statistical analysis controlling for primary psychiatric diagnosis and severity, patient age, or patient sex and whether these variables contributed to instances of CG or RS.
Our primary goal of exploring a potential link of statin use to aggression led to a secondary detection of significant unexplained deviations from current statin guideline recommendations involving calculated ASCVD risk and intensity of statin prescribed, thus warranting further independent evaluation. The number of CGs and RSs each patient required were only counted during the first year of admission for our control group as this is when patients are likely to be the most psychiatrically unstable. Total cholesterol levels used during this analysis were within one year of admission in order to match statin initiation date and CG/RS time period. This ensured the comparison between statin therapy, cholesterol level, and aggression was well matched and could be extrapolated to other psychiatric patients.
Only total cholesterol levels were assessed during this analysis because not all patients had complete fasting lipid panels (FLPs); the majority of hospitalized patients only had total cholesterol and triglyceride levels available. Future analysis could assess whether LDL levels contribute to increased risk of aggression in psychiatric inpatients, considering statin therapy does primarily impact LDL level. Future analysis could be beneficial in examining at what total cholesterol level does the risk of aggression increase because this was not assessed during our analysis.
The ANOVAs suggested that total cholesterol levels, and not statin therapy, were associated with increased CGs/use of RS. Our analysis demonstrates that increased aggression in psychiatric patients is very likely not a result of statin therapy, but instead a lower total cholesterol level, whether driven by statin therapy or by natural propensity. It appears that psychiatric patients with lower total cholesterol levels could be at an increased risk for loss of behavioral control aside from mitigation with both psychiatric medications and the inpatient milieu.
Conclusion
Recent trials and literature were specifically evaluated for behavioral changes associated with statin use. While cardiovascular benefits of statin medications have resulted in increased overall statin prescribing in the United States, it has been noted that psychiatric inpatient providers might be cautious, often deviating from guideline protocol, when prescribing statin therapy to inpatient psychiatric patients, possibly due to the concern of potentiating increased aggression. Further investigation is warranted to determine if other potential factors influence non-standard statin prescribing trends in a psychiatric population. Low or lowered cholesterol has been linked with low serotonin activity, which can result in increased depression, violence, and impulsivity. Our analysis suggests that statin therapy alone does not increase patient aggression. However, it is unclear whether rapid lowering of cholesterol or simply having low cholesterol levels contribute to the observed psychiatric changes, and further research in this area is needed. More studies need to be completed before determining if statin prescribing should be changed in psychiatric patients.
References
- Cham S, Koslik HJ, Golomb BA. Mood, personality, and behavior changes during treatment with statins: a case series. Drug Saf Cas Rep. 2016;3(1):1.
- Golomb BA, Kane T, Dimsdale JE. Severe irritability associated with statin cholesterol- lowering drugs. QJM. 2004;97:229–35.
- Tatley M, Savage R. Psychiatric adverse reactions with statins, fibrates, and ezetimibe: implications for the use of lipid-lowering agents. Drug Saf. 2007;30:195–201.
- Tuccori M, Lapi F, Testi A, et al. Statin-associated psychiatric adverse events: a case/noncase evaluation of an Italian database of spontaneous adverse drug reaction reporting. Drug Saf. 2008;31:1115–23.
- Sahebzamani FM, D’Aoust RF, Friedrich D, et al. Relationship among low cholesterol levels, depressive symptoms, aggression, hostility, and cynicism. J Clin Lipidol. 2013;7(3):208–16.
- Muldoon MF, Manuck SB, Mendelsohn AB, et al. Cholesterol reduction and non-illness mortality: meta-analysis of randomized clinical trials. BMJ (Clinical Research Ed). 2001;322:11–5.
- Golomb BA. Cholesterol and violence: is there a connection? Ann Intern Med. 1998;128:478–87.
- Golomb BA, Stattin H, Mednick S. Low cholesterol and violent crime. J Psychiatr Res. 2000;34:301–9.
- Conklin SM, Harris JI, Manuck SB, et al. Serum omega-3 fatty acids are associated with variation in mood, personality and behavior in hypercholesterolemic community volunteers. Psychiatry Res. 2007;152:1–10.
- Littarru GP and Langsjoen P. Coenzyme Q10 and statins: biochemical and clinical implications. Mitochondrion. 2007;7 Suppl: S168–74.
- Golomb BA, Dimsdale JE, Koslik HJ, et al. Statin effects on aggression: results from the UCSD statin study, a randomized control trial. PLoS One. 2015;10(7):e0124451.
- Walker ER, McGee RE, Druss BG. Mortality in mental disorders and global disease burden implications: a systematic review and meta-analysis. JAMA Psychiatry. 2015;72(4): 334–341.