
 by Dharmendra Goyal, MBBS; Sandarsh Surya, MBBS; Joshua Elder, MD; William V. McCall, MD; and Krystle Graham, DO
by Dharmendra Goyal, MBBS; Sandarsh Surya, MBBS; Joshua Elder, MD; William V. McCall, MD; and Krystle Graham, DO
All authors are with the Department of Psychiatry and Health Behavior, Medical College of Georgia, Georgia Regents University in Augusta, Georgia, USA.
Innov Clin Neurosci. 2016;13(1–2):40–42.
Funding: No funding was received for the preparation of this manuscript.
Financial Disclosures: The authors have no conflicts of interest relevant to the content of this article.
Key Words: Trichotillomania, sleep, alcohol, NREM, clomipramine, and SSRIs
Abstract: We report a case of sleep-isolated trichotillomania admitted to the hospital for alcohol detoxification. It would be helpful for patients with sleep-isolated trichotillomania to have diagnostic polysomnography to identify any other sleep-related pathology and correlate sleep-isolated trichotillomania behaviors with the sleep cycle to identify specific treatment for sleep-isolated trichotillomania.
Introduction
Trichotillomania (TTM) is a recurrent irresistible urge to pull one’s own body hair, and is classified in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) as an obsessive compulsive disorder (OCD).[1] Sleep-isolated trichotillomania (SITTM) is defined as the plucking of body hairs during sleep with no recollection of the event while awake.[2,3] Only two cases of SITTM have been published—one case suggested that hair pulling at night may be a nonrapid eye movement (NREM) sleep parasomnia.[2] The second case reported that the patient had nonepileptic seizures, and that the TTM may be a symptom of a sleep-related dissociative disorder.[4]
TTM can lead to evident alopecia and is associated with social and functional impairment. It affects four percent of the population, with the estimated lifetime prevalence of 1.5 percent (males) and 3.4% (females).[5,6] The prevalence rates are approximately equal among male and female ages 9 to 13 years.[7] Adults have a chronic course associated with other psychopathology in 53 percent (23%: major depression; 23%: generalized anxiety disorder, and 26%: OCD), while children and adolescents have a benign course.[8] TTM may present grossly with patchy alopecia and can be diagnosed with characteristic trichoscopy findings including blunt-tipped hairs. The etiopathology of TTM is complex; various studies and cases reported that TTM has genetic and familial basis.[9]
We report a case of SITTM in a patient hospitalized for treatment of alcohol use disorder.
Clinical Vignette
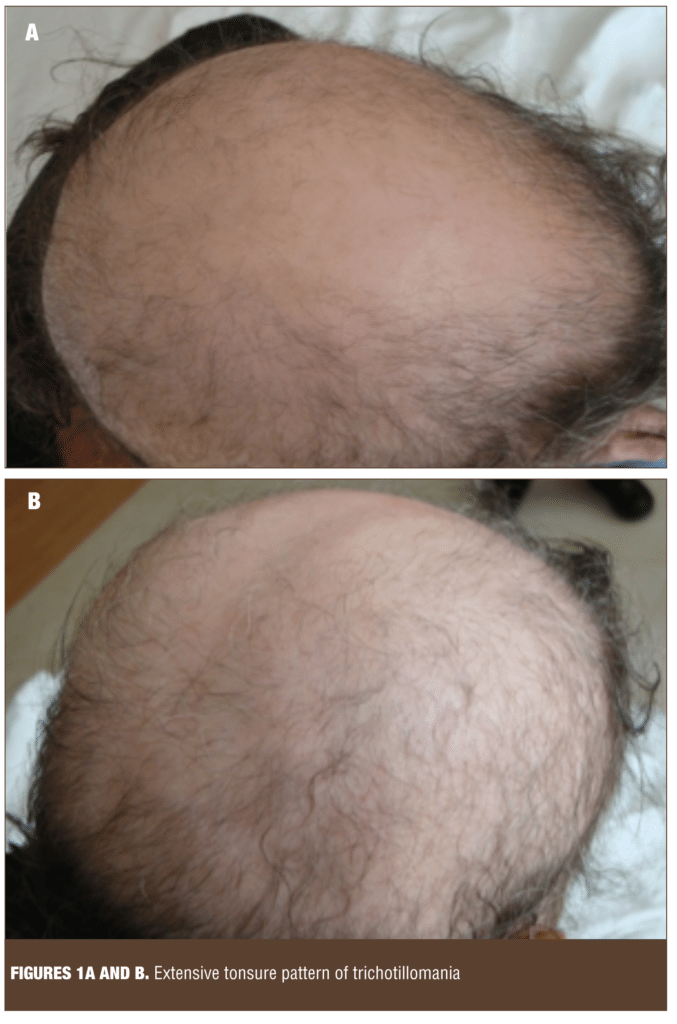
A 44-year-old Caucasian woman with a 17-year history of alcohol use was admitted to the inpatient psychiatric service for alcohol detoxification. The patient asked staff upon admission for a surgical cap and wore it at all times during her hospitalization. On further inquiry, she reported a long history of TTM beginning around age five. The patient denied a history of direct sexual or physical abuse, but she attributed the onset of her behavior to witnessing domestic abuse between her parents at a young age. She reported her hair pulling behavior began during early childhood and that it occurs during sleep 2 to 3 times a month (Figures 1A and B). She could not remember the episodes but would see hairs on the pillow and on the bed next morning. She mentioned that these episodes got worse when she felt anxiety at night. She reported no use of nicotine, caffeine, or zolpidem in the evening or night. She reported that she would go to sleep around 10pm and that it would take around half an hour for her to feel sleepy, sometimes two hours because of feeling anxiety at bedtime. Her husband reported that occasionally she would experience nightmares and vivid dreams in which she had dramatic conversations. Her husband also reported that the patient had a history of sleepwalking, and that she moved both arms in the air while asleep, sliding one arm over the other alternatively. The patient mentioned that her father and grandfather used to do the same arm movements during sleep. No abnormal leg movements were noticed by the husband. She would snore occasionally but had no history of apneic episodes; she would feel sleepy during the day but did not take naps. Epworth Sleepiness Scale score was 8. Her history was not significant for depression, mania, or psychosis. Her PTSD Checklist—Civilian Version (PCL-C) score was not sufficiently abnormal to suggest posttraumatic stress disorder (PTSD), but was significant for symptoms of hypervigilance, avoidance of thinking or talking about stressful experiences, and avoidances or activities that would remind her of the past, nightmares, memories, thoughts, and images. Similarly, her Yale-Brown Obsessive Compulsive Scale score did not suggest OCD or other related disorders. The family history was significant for alcoholism in both parents, and her mother had a history of an extensive nail biting habit. Our patient was treated for alcohol withdrawal and started on fluoxetine for the trichotillomania. She was seen in an outpatient clinic after one month of the hospital discharge. The patient said that fluoxetine did not help much and that she had discontinued the medicine. She was lost to follow up after that appointment.
Discussion
TTM is an established psychopathology, but SITTM is a relatively underreported condition. The first-line treatment for TTM is cognitive behavioral therapy plus selective serotonin inhibitors (SSRIs) or clomipramine. The number of reported cases of SITTM is insufficient to determine underlying etiology and or make specific treatment recommendations. One case report suggested that SITTM is a NREM sleep parasomnia. Future investigations of patients with SITTM should consider pursuing polysomnography to rule out sleep-disordered breathing, confusional arousals, other NREM parasomnias, and REM behavior disorder.[6] Further identification of such cases is needed to learn about etiology and develop treatments for this disorder.
References
1. Stein DJ, Grant JE, Franklin ME, et al. Trichotillomania (hair pulling disorder), skin picking disorder, and stereotypic movement disorder: toward DSM-V. Depress Anxiety. 2010;27:611–626.
2. Murphy C, Valerio T, Zallek SN. Trichotillomania: An NREM sleep parasomnia? Neurology. 2006;66:1276.
3. Murphy C, Redenius R, O’Neill E, et al. Sleep-isolated trichotillomania: A survey of dermatologists. J Clin Sleep Med. 2007;3:719–721.
4. Angulo-Franco M, Bush-Martínez A, Nenclares-Portocarrero A, et al. Trichotillomania and non-epileptic seizures as sleep-related dissociative phenomena. J Clin Sleep Med. 2014;pii:jc-00331-14.
5. Huynh M, Gavino AC, Magid M. Trichotillomania. Semin Cutan Med Surg. 2013;32:88–94.
6. Ko SM. Under-diagnosed psychiatric syndrome. I: Trichotillomania. Ann Acad Med Singapore. 1999;28:279–281.
7. Tay YK, Levy ML, Metry DW. Trichotillomania in childhood: Case series and review. Pediatrics. 2004;113:e494–498.
8. Woods DW, Flessner C, Franklin ME, et al. Understanding and treating trichotillomania: What we know and what we don’t know. Psychiatr Clin North Am. 2006;29:487–501.
9. Flessner CA, Knopik VS, McGeary J. Hair pulling disorder (trichotillomania): genes, neurobiology, and a model for understanding impulsivity and compulsivity. Psych Res. 2012;199:151–158.