
 by Ivan Sascha Sheehan, PhD
by Ivan Sascha Sheehan, PhD
Dr. Sheehan is Graduate Program Director and Assistant Professor, Negotiation and Conflict Management Program & Global Affairs and Human Security Program, School of Public and International Affairs, University of Baltimore, Baltimore, Maryland.
Innov Clin Neurosci. 2014;11(9–10):81–92
Funding: There was no funding for the development and writing of this article.
Financial Disclosures: Dr. I.S. Sheehan is the co-author with Dr. D.V. Sheehan of the Sheehan-Homicidality Tracking Scale (S-HTS).
Key Words: Suicide, terrorism, suicide terrorism, suicide attacks, suicide missions, martyrdom operations
Abstract: Objective: Most of the research on suicide terrorism is conducted in the political science and international relations fields. The prevailing wisdom within this literature is that suicide terrorists are not suicidal. But how good is the evidence for this assumption? Knowing whether suicide terrorists are suicidal has implications for prevention, rehabilitation, and the “softer” side of counterterrorism designed to win minds and hearts. In addition it may deepen our understanding of suicide itself. Design: This article uses a review of existing literature to examine the arguments and evidence for and against the possibility that suicide terrorists could be suicidal in the context of a broad range of explanations for suicide terrorism. Results: Much of the evidence against the possibility that suicide terrorists are suicidal is based on anecdote or faulty assumptions about suicide. Relatively few formal systematic studies of suicidality in suicide terrorists have been conducted. Nonetheless, there is emerging evidence that suicidality may play a role in a significant number of cases. Conclusion: The field needs a more multidimensional approach, more systematic data at the individual level, and greater international cross-disciplinary collaboration. Would-be suicide terrorists (intercepted and arrested on their way to an attack) should be routinely interviewed using standard internationally accepted psychiatric diagnostic interviews as well as suicidality and homicidality rating scales. Psychological autopsies should also be routinely conducted worldwide. Since no one research site can collect all of the information that is needed, the creation of an internationally shared database that focuses on suicide terrorists rather than simply incidents is encouraged.
Introduction
Suicide terrorism is the most lethal form of terrorism. Unfortunately, it is on the increase. In 2013 alone, some 384 suicide terrorist acts were carried out in 18 countries causing 3,743 deaths. This represented a 46-percent growth over the number of attacks in 2012 and a 66-percent increase in the number of lethal casualties.[1]
What drives suicide terrorism and to what extent is suicidality a contributing factor? Although suicide terrorist acts have become disturbingly frequent, with more than 3,500 since 2003,[1] we still know very little about the individuals who commit them.
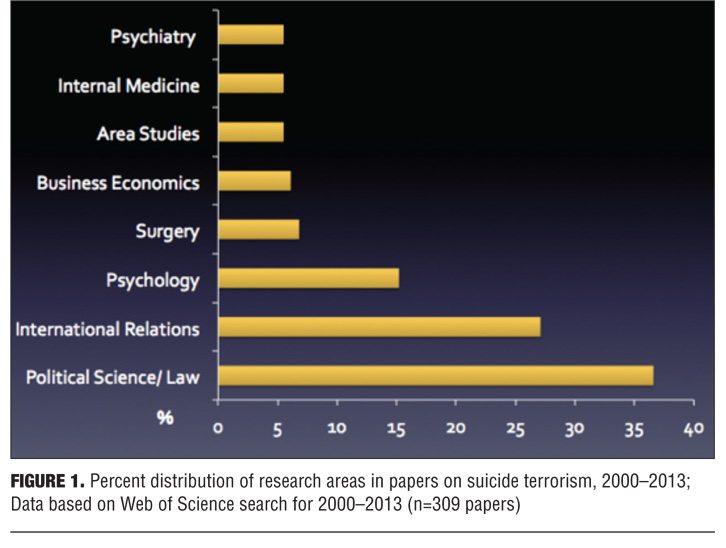
As shown in Figure 1, most of the scholarship on suicide terrorism (63%) comes from the political science and international relations fields (Figure 1). By contrast only a small proportion originates in disciplines that focus on the individual, such as psychology (16%) and psychiatry (5%). Within this literature, the conventional wisdom is that suicide terrorists are normal, well-adjusted individuals who turn to suicide terror for political or religious reasons or simply because of social and group processes. But how good is the evidence for these claims and to what extent are arguments for and against suicidality as a contributing factor to suicide terrorism supported theoretically?
This article reviews existing scholarship to try to answer these questions. A basic assumption behind the article is that suicide terrorism is a multifaceted problem that needs to be approached from multiple perspectives at multiple levels: the society, the group and the individual who volunteers for the mission in the first place.
Background
Definitions. Suicide terrorism, sometimes labeled “suicide attacks,” “suicide missions,” “suicide operations,” but also “martyrdom operations,” has been defined as “the targeted use of self-destructing humans against noncombatant—typically civilian—populations to effect political change.[2] Typically, it is viewed as a “weapon of psychological warfare intended to affect a larger public audience” (i.e., those who are “made to witness it”).[2] The audience may be a government, the group’s own domestic supporters, rivals, potential patrons, or a diaspora.
In some definitions, the death of the perpetrator is required. For example, Dr. Boaz Ganor, Executive Director of the International Policy Institute for Counter-Terrorism in Israel, defines suicide terrorism as “an operational method in which the very act of the attack is dependent upon the death of the perpetrator.”[3] University of Massachusetts professor Mia Bloom also asserts that the perpetrator’s death “is the precondition for the success of the attack.”[4] Robert Pape of the University of Chicago, however, only requires that “the attacker does not expect to survive the mission” while Ami Pedahzur of Haifa University clarifies that the odds of returning alive are “close to zero.”[5,6] For Ariel Merari of Tel Aviv University, what is critical is the “readiness to die in the process of committing a terrorist act.” This means that unintended suicides (cases in which the attacker is coerced into detonating a suicide belt, for example, or cases in which the driver of a bomb-laden car is not told ahead of time that he will die in the mission) are not counted as suicide terrorism. However, acts that are intercepted or interrupted or fail are counted if the perpetrator is willing to kill and die in the process.[7]
Myths and history. In the aftermath of the September 11, 2001, terrorist attacks on New York City and Washington, DC (9/11), two myths were routinely promoted: 1) suicide terrorism was a new phenomenon and 2) it was almost always the province of religious fanatics. In fact, suicide terrorism has existed since ancient times. Nor does any society or religion have a monopoly on it. The Zealots, a Jewish sect, practiced suicide terrorism in Rome-occupied Judea as early as the first century. Typically, a Zealot, also called Sicari or “daggerman,” would go up to a Roman soldier and stab him in front of other soldiers knowing full well that he would be executed on the spot. The Islamic Order of Assassins also used suicide operations in the region we now know as Syria as far back as the Crusades in the 12th century.[8] More recently, suicide operations have been carried out by a variety of secular groups including the Anarchists in 19th century Russia and the Liberation Tigers of Tamil Elam (LTTE), a leftist Marxist group in Sri Lanka, who became the world leaders in suicide terrorism in the 20th century.[9] Suicide terror has also been sponsored by sovereign states. In the Battle of Okinawa (April 1945), for example, Japan dispatched some 2,000 kamikaze who rammed fully fueled fighter planes into more than 300 ships, killing 5,000 Americans in the most costly naval battle in United States history.[10] Iran too sent waves of young volunteers on suicide missions, in this case against the then United States-backed Iraqi army in the Iran-Iraq War of the 1980s, and Iran is now believed to have sponsored the first major modern suicide operation, namely the bombing of the Iraqi embassy in Beirut in 1981. This event is viewed as a landmark in suicide terrorism since explosives were deliberately carried to the target and delivered by surprise—it left 27 dead and over 100 wounded. Iran is also believed to have been behind the truck bombing of the Marine barracks bombing the following year—an attack that killed almost 300 American and French servicemen and drove President Reagan to withdraw forces from Lebanon. That attack served as a model for the devastating 9/11 suicide attacks, this time using airplanes driven into buildings.
Recent trends. Suicide terrorism is not new, nor is it necessarily a religious phenomenon. The problem, however, has escalated in the last decade. As shown in Figure 2, the number of suicide attacks worldwide rose from an average of five per year in the 1980s to 10 per year in the 1990s. It continued to climb after 9/11, reaching a peak of 521 in 2007 at the height of the Iraq War. While the frequency of these attacks began to decline in 2008, suicide operations have been on the upswing again since 2012 reaching a height of 384 in 2013, a 46-percent increase over 2012.[1]

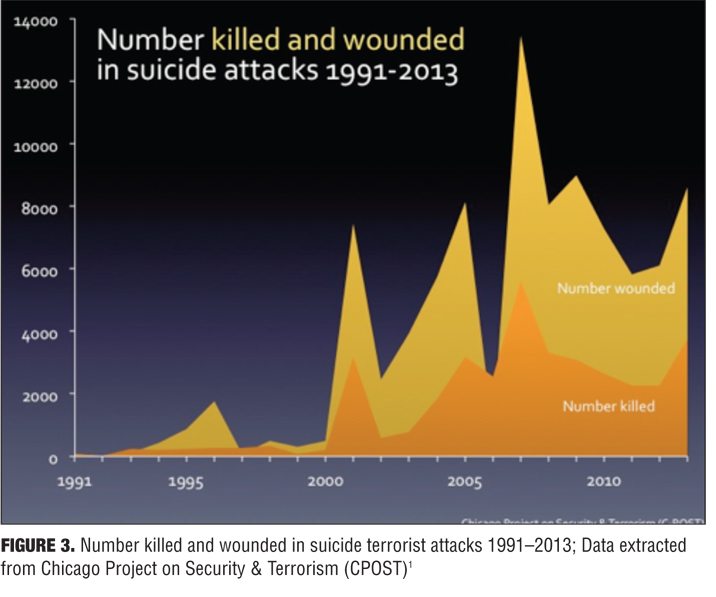
These trends are worrisome since suicide terrorism is the most lethal form of terrorism, 13 times deadlier than any other form of attack.[5] Overall, suicide attacks have taken the lives of more than 37,000 since 1991 and wounded more almost 102,000. Moreover, as shown in Figure 3, the number killed increased by a factor of 18 and the number wounded grew by a factor of 17 in first decade of the 21st century (Figure 3).[1]
Explanations
What accounts for suicide terrorism? Why has it increased so dramatically in the last decade? Social scientists have tried to explain the phenomenon at three general levels of analysis: the political/strategic, the social/cultural, and the personal.
National liberation. Robert Pape, Director of the Chicago Project on Suicide Terrorism, makes the claim that suicide operations are almost always rational and strategic. Specifically, he argues that such attacks are designed to coerce an adversary and drive occupiers out of a homeland. “Every group mounting a suicide campaign over the past two decades has had as a major objective […] coercing a foreign state that has military forces in what the terrorists see as their homeland to take those forces out.”[5]
How well does this theory stand up to the empirical evidence? The tactical benefits of suicide terrorism are well known. Suicide attacks are cheap. Estimates vary, but the operation may cost as little as $150 per attack.[11] This kind of attack can be mounted anywhere and the perpetrator can easily pivot and change direction without having to make elaborate escape plans. Suicide attacks are also effective in that they kill many more people than other kinds of attacks. According to one estimate, the average number of victims from a suicide truck or car bombing is 30 times higher than the number from a shooting (97.8 vs. 3.3) and 14 times higher than the number from a remote-control explosive attack.[5] As a result suicide operations create a spectacle, bringing attention to a cause.
But is suicide terror always designed to expel an occupier from a homeland? Professor Pape uses over 300 cases to support his theory. He points out that that Hezbollah, with the support of Iran, used campaigns of suicide attacks to drive the United States and France out of Lebanon, that the LTTE used suicide operations to get Sri Lanka to accept a Tamil State, that Palestinian groups used suicide attacks to try to get Israel out of the West Bank and Gaza, that Chechen rebels also used the same modus to get Russia out of Chechnya, and al Qaeda fits the model insofar as one idea behind the 9/11 attacks was to get the United States to withdraw from Arab heartlands including Saudi Arabia, Iraq and Palestine. One could argue that the Taliban fits this model too as is evident in a 2013 headline, “Taliban vow suicide and “insider” attacks in new spring offensive.”[12]
Pape’s theory is not without flaws. One problem is that not all countries that are occupied produce suicide attackers. There is the additional problem that many suicide attackers come from countries that are not occupied. Consider the Madrid bombers, the London bombers, the waves of young people from countries such as Indonesia, Saudi Arabia, Morocco, and other non-occupied lands who flocked to Iraq and Afghanistan to conduct suicide operations. These trends have led to growing skepticism about the merit of seeing suicide terrorism as a strategy of national liberation.
As Atran puts it, “When Arabs from more than a dozen countries rush to embrace death in Iraq to kill Shi’as who are probably more supportive of Iran than the United States, it is quite a stretch to identify the common thread as a secular struggle over foreign occupation of a homeland unless “secular” covers transcendent ideologies, ‘foreign occupation’ includes tourism, and ‘homeland’ expands to at least three continents.”[13]
The general theory that suicide terrorism is always rational and strategic has also come under attack. Brym and Raj, for example, observe that the during the Second Intifada, “the objectives and precipitants of suicide bombing reveal little of the strategic logic that, according to Pape, lies at its core.” Indeed they claim that retaliation for specific Israeli actions was more pertinent, and, in this case, suicide tactics could hardly be considered rational since they resulted in so many arrests, assassinations, and other collateral damage.[14]
Gaining an edge over rivals. Mia Bloom, while agreeing that suicide terror is often a strategy of liberation, observes that its attraction may lie, in addition, in the prestige it confers. In particular, she notes that suicide terrorism can give a group an advantage over rivals in terms of recruitment, publicity, and money. Bloom uses the example of the Popular Front for the Liberation of Palestine (PFLP), a group that turned to suicide terrorism only after it realized that Hamas had gained in popularity and recruitment when it engaged in suicide terrorism.[15] Others, however, have raised questions about the extent to which market share plays a significant role. Crenshaw, for example, observes that the most vigorous suicide campaigns of the LTTE occurred well after the group had eliminated most of its competition and al Qaeda’s actions too are “hard to explain in terms of competition with rivals.”[16]
Poor economic development. Political leaders have long claimed that poverty breeds terrorism. The evidence to support this claim, however, is weak. Princeton economist Alan Krueger and his colleague Jitka Maleckova found no correlation between poor economic conditions and terrorism. Indeed their research indicated that Palestinian suicide attackers came from wealthier families and had higher levels of education than those of average Palestinians.[17] These results are supported by others. Harvard professor Albert Abadie, for example, found that while the freest and richest countries have experienced the least terrorism, this is also true of the poorest and most oppressed.[18] James Piazza’s findings are consistent with these results.[19] On the other hand, Efraim Benmelech and colleagues at Harvard have produced more nuanced findings showing that while economic conditions are not associated with the quantity of terror, they may impact its quality. In particular, they note that poor economic conditions may lead more able, better educated individuals into terror attacks, allowing organizations to send the best qualified to the highest impact terrorist missions.[20]
The pull of cultures of martyrdom. Mohammad Hafez of the University of Missouri, among others, has called attention to the pull of “cultures of martyrdom” as a contributing factor in suicide operations.[21–23] There is no question that some terrorist groups consciously cultivate cultures of martyrdom and promote them in a “top-down” way to draw recruits. Hamas calendars, for example, herald the “Martyr of the Month.” Similarly the LTTE and Turkey’s Kurdistan Workers party (PKK), both secular groups, celebrate the anniversary of their first suicide bombers every year, while Chechen groups are known to commemorate the first Chechen suicide bomber in a popular song.[24] The extent to which consciously created cultures of martyrdom play a role in suicide operations, however, may be overstated.
The pull of social networks and ties. Others have suggested that suicide terrorism is better explained as a “bottom-up,” leaderless group or cultural phenomenon. Mark Sageman, a forensic psychiatrist and former intelligence officer, studied the biographies of more than 400 members of so-called Islamic terrorist groups with ties to Al Qaeda. In particular, he looked at ones who joined extremist Salafi groups. What he found was that many were uprooted, living away from their homelands, often away from family, in countries where they suffered insults and humiliation for being foreign and, for that matter, for being Arab. They joined groups that espoused suicide terrorism largely because their friends joined. Many went off to missions in friendship pairs, sibling pairs, husband and wife pairs, and even parent/child pairs. In one case, 8 of 11 members of a Hamas-associated football club carried out suicide attacks.[25] Building on Sageman’s work, Atran put forward the theory that being part of a group that encourages camaraderie and conforming to the group may be the most important motivator for suicide terror especially in diaspora communities.[26]
But again how good are these theories? Cultural and small group theories, while compelling, still do not explain why some of those who join terror groups strap on bombs and kill themselves while others take on other roles (e.g., as organizers, recruiters, or reconnaissance). What differentiates the ones who actually strap on a bomb to kill themselves?
This brings us to explanations at the personal and psychological level. Here there is quite a bit of controversy.
Personal motivations. Suicide attacks are almost always organized by groups that recruit, train, and provide logistics (e.g., time, place, target, and weapon). At the same time, the suicide terrorist actor belongs to what Ariel Merari and colleagues call a “select group.”[27] Whether there is social support, and some societies are more supportive of suicide operations than others,[28] the individual still has to make the irretrievable decision to participate in the act. What distinguishes those who do?
Despair, humiliation, injustice. Harvard’s Jessica Stern has argued that suicide terrorists are almost always driven by a sense of humiliation and injustice.[8] Hafez places the act in the context of an escalating sense of victimization. Similarly, Atran emphasizes feelings of “injustice” and “humiliation” as driving factors.[2]
Loss and revenge. For individual perpetrators of suicide acts, there may be an additional desire for personal revenge after the loss of a loved one. Sageman, in his work on extremist Salafi groups, found that nearly all of those he studied had someone close to them suffer injury or death.[25] Anne Speckhard reports that among the female suicide bombers in Chechnya she studied, most were widows or bereaved siblings.[30] Others have found that significant proportions of suicide attackers suffered other losses at the hands of an enemy. Based on post-mortem results, Rona Fields and her coauthors, for example, found that five of the nine suicide terrorists they examined had been injured as a result of the intifada in Gaza. Eight had been imprisoned and tortured, and in five of the eight, their families had been reportedly beaten and humiliated by soldiers.[31]
Material incentives. Material incentives, including cash, free apartments, and the guarantee of a place in heaven, have also been cited as playing a role.[9]
Are They Mentally Ill?
The general consensus among scholars is that suicide terrorists do not have significant psychopathology.[2,5] But how good is the evidence for this claim?
Most of the “evidence” is impressionistic. Based on interviews with 250 Palestinian suicide terrorist recruiters, trainers, and would-be suicide bombers and their families, Nasra Hassan of the United Nations Office on Drugs and Crime simply asserts that suicide bombers seem to be normal: “They all seemed to be normal members of their families. They were polite and serious; and in their communities they were considered to be model youth.”[32]
Using case studies designed to examine the strategic motivations behind suicide attacks, Robert Pape makes similar claims: “Few suicide attackers are social misfits, criminally insane or professional losers […] Most are deeply integrated into social networks and emotionally attached to their communities.”[5]
In a similar vein, Riaz Hassan of Flinders University asserts that “the causes of suicide bombings lie not in individual psychopathology but in broader social conditions.”[33]
A few scholars simply note that suicide terrorist recruiters “screen out” the mentally unstable—as if that closes the case.[34,35]
Others, however, have provided anecdotal evidence that suggests that such screens may not be successful, if they are conducted at all. Reporting on her interviews with the families of female suicide bombers in Chechnya, the West Bank, and Gaza, Lisa Ling notes that many had lost a husband or close relative in the war and most were “vulnerable broken women who saw no way out.”[36] Similarly, Brian Glyn Williams, in his study of suicide attacks in Afghanistan, notes that Afghan police told him that large numbers of suicide bombers the police arrested after failed suicide bombing attempts were “mentally unsound, deranged” or cognitively impaired.[37] Others have supported these claims.[38] According to Yusef Yadgani, a pathologist at Kabul Medical University, three of every five suicide bombers he studied in his lab had a physical ailment or disability. Adding those who suffer from mental illness, the number of sick and disabled bombers climbs to more than 80 percent in his estimate.[39]
To date, relatively few formal studies of psychopathology in suicide terrorists have been published, and the results are mixed. University of Toronto professors Robert Brym and Bader Araj conducted 42 sets of in-depth semi-structured interviews with the immediate family members and friends of a random sample of suicide bombers who died in suicide missions in the West Bank and Gaza. Using a battery of questions and documentary evidence, they found that although 21 percent of the bombers had expressed a desire for martyrdom, 76 percent did not manifest any outward sign of depression or personal crisis in the year preceding the attack. While 24 percent did show outward signs of depression, this rate, they claim, was not unusually high given population statistics for depression in the West Bank and Gaza.[41] This evidence, however, has limitations. As Ariel Merari observes, information from family and friends may be “skewed by the wish to present them in a positive light.”[41] In addition, as the authors themselves observe, “loved ones can be oblivious to the internal turmoil” of the person engaging in these acts.[41]
Somewhat different results were obtained by Anne Speckhard of Georgetown University and her colleague Khapta Akhmedova in their study of 26 female Chechen suicide bombers. Based on interviews with family members and close associates, they found that nearly all had lost close family members in air raids, bombings, or landmines carried out by Russian forces and in battle. Many had personally witnessed death or beatings of family members at close hand. According to their family members and friends, none had significant personality disorders or psychiatric symptoms before the trauma, but all changed afterwards. In particular, all had dissociative symptoms characteristic of posttraumatic stress disorder (PTSD). In addition, in the period before they engaged in suicide terrorism, three fourths (73%) showed signs of depression, 92 percent became socially isolated, 23 percent became aggressive, and 31 percent began talking repetitively about “revenge.”[42]
The latter results are supported in a controlled study of “would-be” suicide terrorists by the Israeli psychologist Ariel Merari. Merari interviewed 15 would-be suicide terrorists (intercepted moments before their attacks), 12 nonsuicide terrorist matched controls, and 14 terrorist organizers. None of the subjects had a diagnosis of psychosis or a history of hospitalization for mental disorders. Eight (53%) of the would-be suicide terrorists displayed symptoms of depression—melancholy, sadness, hopelessness, low energy, tearfulness, emotional constriction, and distracted attention. In addition, three of the would-be suicide terrorists, but no controls, had evidence of PTSD. In contrast, only three of the organizers (8%) had depressive tendencies and none of the controls or organizers had evidence of PTSD. Merari also found a much higher incidence of dependent avoidant personality in the would-be suicide bombers (69%) compared to controls (20%) and organizers (8%). As another difference, he found that while three of the controls (25%) and one organizer (7%) exhibited psychopathic tendencies, none of the suicide bombers showed these traits.[27] These results are supported by case studies of deceased suicide bombers conducted by University of Alabama criminal justice professor Adam Lankford.[43]
Are They Suicidal?
Arguments against suicidality as a contributing factor. The prevailing view among scholars is that suicide terrorists are not suicidal. Again, how good is the evidence? Ellen Townsend of University of Nottingham argues that suicide terrorists are not suicidal based on the following propositions: 1) suicide is associated with psychopathology, and suicide terrorists do not exhibit overt psychopathology; 2) recruiters screen out the mentally ill; 3) suicide using violent methods is an impulsive act while suicide terrorism is meticulously planned; 4) suicide terrorism has murderous intent, and murderous intent is rare in suicide; 5) many suicide terrorists are religious, but religion protects against suicide.[44] Another assumption that is sometimes made is that suicide terrorists could not be suicidal since suicide terrorists often act in familial networks of relative pairs (siblings, parent-child, or cousin pairs) and such acts are more likely to be a result of socialization and family bonds. How well do these arguments hold up?
Psychopathology argument. The proposition that suicide terrorists could not be suicidal because they have no psychopathology has clear flaws. It is true that psychopathology is the most important antecedent and correlate of suicidal behavior worldwide.[45] However, as Brooke Rogers and colleagues of Kings College London observe, studies on the psychopathology of suicide terrorists have not been systematic and what evidence does exist is mixed.[46] It is possible that psychiatric disorders such as depression and PTSD are higher in this population than is generally assumed. To complicate matters, the precise role of psychopathology in suicide is not as straightforward as might appear. Indeed, there is increasing evidence from twin studies that while psychopathology is often associated with suicide, susceptibility to suicidal ideation and behavior may be transmitted genetically independently of the presence of a psychiatric disorder.[47] There is growing evidence, moreover, that suicidality is associated with a long list of medical and psychiatric disorders, and that it is not always associated with depression as is popularly assumed.[48] These findings have led to the suggestion that suicidality may be made up of several primary disorders that can be comorbid but are independent of other psychiatric disorders.[49,50] In support of this view is the finding that in the treatment of depression medication may make suicidality worse in some, better in others, and have no effect in a third group. On the other hand, some medications associated with suicide reduction (e.g., lithium and clozapine) are not indicated or approved for the treatment of depression.[51–54]
Recruitment argument. The assumption that recruiters successfully reject candidates who are mentally ill is also problematic. It’s not just that recruiters may actually seek out depressed candidates—Anat Berko in her interviews in Israeli prisons found that, contrary to the conventional wisdom, dispatchers are often told to “look for sad guys.”[55] Nor is it just that we have anecdotal evidence, at least from Afghanistan, that many of those who are recruited are “mentally challenged.”[37] There is an additional problem. How exactly do these recruiters actually screen out the mentally ill? What tools do they use and to what extent are they influenced by cultural frames?
Cultural frames may be particular barriers for recruiters in the context of Islamic terrorist recruitment. Okasha and Okasha observe that religious people in the Muslim world often miss psychiatric symptoms or interpret them from a religious perspective. For example, negative signs of psychosis (withdrawal, poverty of thought) may be interpreted in terms of piety while positive ones (auditory or visual hallucinations) are viewed as “gifts of God.”[56] The express focus of recruiters on finding candidates with high motivation and a sense of duty may also backfire. In fact, there is good evidence that these very traits, together with lack of help-seeking, are the ones that best predict suicidal behavior in soldiers in combat situations.[57]
Impulsivity argument. The notion that suicide terrorists could not be suicidal because their acts are meticulously planned and suicide is impulsive is simply wrong. While impulsive traits have been shown to increase the risk of suicide in some populations, especially those with bipolar disorder and alcohol abuse, decades of research have shown that the majority of those who commit suicide do not do so impulsively and, in fact, have had suicidal ideation for some time and made prior plans for these acts.[58,59]
Murderous intent argument. The proposition that suicide terrorists could not be suicidal because they have murderous intent represents a false dichotomy. Even if suicide terrorists have murderous intent, that fact does not mean that they cannot also have suicidal intent. They may be both suicidal and homicidal. And, depending on the culture in which the act occurs, the degree of homicidal intent may be higher or lower. Williams notes that, at least in the initial phases, suicide attacks were less effective and took fewer victims in Afghanistan than in Iraq. This may be because of cultural taboos on killing innocents in Pashtun culture.[37]
Religiosity argument. Finally, the notion that suicide terrorists cannot be suicidal because many are religious and religion protects against suicide is debatable on several counts. First, not all suicide terrorists are religious. Many are secular. The Palestinian Fatah, the PFLP, and the PKK, for example, have little or no connection to fundamentalist Islam. Moreover, one of the terrorist organizations that have regularly employed suicide terrorism as a strategy in modern times is the LTTE. Not only are members of this organization not Muslim, most of them are not religious at all. Second, the protective power of religion in preventing suicide may be overstated.[60] It is true that religious affiliation has been found to be associated with lower rates of suicide attempts in some clinical populations.[61,62] These findings, however, may be biased since disclosure of suicidal ideation and behavior might be lower in people with religious affiliations because of the taboos against it.[63–65] In relation to Islam specifically, Okasha and Okasha note that suicide is forbidden by the Qu’ran, and few Muslims will admit to suicidal behavior when questioned directly although they will do so when the questions are open-ended.[56] Taboos against suicide can result in underreporting of suicide,[66] and there is growing evidence that suicide is underreported in Muslim countries. For example, in an analysis of suicide and undetermined deaths in 17 predominantly Islamic countries, Pritchard and Amanullah report that reclassification of suicides to include “hidden suicides” (otherwise classified as “other violent death” [OVD]) resulted in the finding that suicide rates in Islamic countries were as high as those in the United Kingdom and at least eight times higher than otherwise officially reported.[67]
Familial network argument. The idea that suicide terrorists could not be suicidal because suicide bombers often act in familial pairs (mother/son, father/daughter, siblings) is problematic in light of growing evidence of genetic factors in suicide.[68] According to one study, identical twins share suicidal tendencies in 15 percent of cases.[69] There is additional evidence from adoption studies showing that the biological relatives of people who commit suicide are six times as likely to commit suicide as members of the families that adopted them.[70] Among individual genes that have been associated with suicide are those involved in the brain’s response to mood-lifting serotonin and a signaling molecule called brain-derived neurotrophic factor (BDNF) that regulates the brain’s response to stress. In a recent study, a group of researchers at MacDill University compared the brains of 46 people who had committed suicide with those of 16 people who died of natural causes. In those who committed suicide, 366 genes, mostly related to learning and memory, had a different set of epigenetic markers—chemical switches that turn genes on and off. These results may be complicated by the fact that many of the people who committed suicide had psychiatric disorders, but the authors found that suicide, rather than the presence of a psychiatric disorder, was the only significant predictor for these specific epigenetic changes.[71]
What the evidence shows. Despite widespread acceptance of the claim that suicide terrorists are not suicidal, the evidence for this claim is weak. Nasra Hassan simply asserts that suicide terrorists she interviewed did not exhibit “suicidal symptoms.”[32] Rex Hudson makes similar claims based on his review of theoretical literature and 12 profiles of terrorists from government archival data.[34] Neither the literature nor the profiles, however, contain any evidence of systematic evaluations of suicidal symptoms. Based on “semi-structured” interviews with 35 terrorists and commanders in Israeli jails, Jerrold Post and colleagues also claim that suicide terrorists are not suicidal. However, they provide little information about the methodology they used to come to this conclusion, relying instead on quotes from terrorist commanders who told them that, unlike suicide, suicide terrorism is istishad (martyrdom or self sacrifice) and that in any case recruiters screen out those who are suicidal.[35]
In the controlled Merari study cited earlier, different results were obtained. Merari found that as many as 40 percent of the would-be suicide bombers, but none of the controls (no-suicide terrorists), displayed suicidal tendencies on a standardized battery of tests; and 13 percent had made previous attempts not related to terrorism. These rates are far in excess of the rates in the general population. In addition, Merari found that 64 percent (9/14) of the organizers said they would never volunteer themselves for a suicide mission.
One of the organizers put it this way: “No, it’s very difficult. Every man has different character and traits. I was destined to organize [suicide attacks] and others were destined to perform martyrdom operations […] I am willing to fight but not to die in a suicide attack. For me life is very basic.”[41]
Another explained: “I wouldn’t be willing to carry out a martyrdom operation. Everyone has his role. I was an organizer.”[41]
On the other hand, a would-be bomber made this statement: “I wanted to kill myself. I used to stand in front of Israeli tanks, hoping they would shoot me. I tried it more than once, but it didn’t work. I didn’t know anymore what to do…Then I met people that offered me the chance to carry out an act of istishhad [martyrdom]. I had been thinking for a long time about an opportunity to die, and when these men showed up, I said to myself that this was a good opportunity.”[41]
Conclusion and Future Directions
The literature on suicide terrorism has been dominated by political and social theories. This may be because the political and social aspects of suicide terror are thought to be more important or at least more pertinent to counterterrorism than individual aspects. It may also be because information on what motivates an individual to engage in this behavior is so difficult to obtain. Suicide terrorists, after all, operate in secret, they are protected by clandestine groups, and many do not live to tell their stories. For scholars, there may be an additional concern—that any inquiry into the psychological or psychiatric aspects of suicide terror somehow marginalizes or deligitimizes the real political and social grievances that are thought to lie at the heart of the pheonomenon.
Emerging evidence that suicidal ideation and behavior do play a role in a “significant minority” of cases of suicide terrorism should not be dismissed. Just because suicidal ideation operates at some level in some cases does not mean that political and social factors do not also operate at other levels or that these levels are not equally important.
What is needed is more systematic, cross-disciplinary research and cross-national collaboration on the subject. The field has benefited from the development of several well organized and systematic databases.[1,72–74] These databases can be mined for factual information about suicide terrorist incidents (when and where they occur, the targets, tactics and weapons used, and the motivations of the groups that promote them). They are not designed, however, to provide insights into the motivations or psychopathology or potential suicide tendencies of individuals who turn to suicide terrorism.
To move the field forward, we need what Sageman has called “an actual terrorist database, not a database based on events or incidents, but on the terrorists themselves.”[75] Given the high lethality of suicide terrorism and the fact that no single organization can collect all the information that is needed, there is a special need for a suicide terrorist database that can be mined and shared internationally.
Major research and healthcare organizations around the world should work together to develop the logistics for such a database. As a first step, such organizations should exert pressure on individual countries to adopt a policy of routinely interviewing “would-be” suicide terrorists (those intercepted and arrested on the way to an attack) using standardized diagnostic interviews for psychiatric disorders, such as the International Neuropsychiatric Interview (MINI),[76] and standardized rating scales, such as the Sheehan Suicidality Tracking Scale (S-STS) and the Sheehan Homicidality Tracking Scale (S-HTS).[77–79] These instruments have the advantage of being brief, very thorough, and easily administered by nonclinicians. The MINI has already been translated into 69 languages, including Arabic and Chinese, the S-STS is available in 25 languages, and efforts are underway to translate the S-HTS. Standardized data collection will allow pooling of data and sharing.
Psychological autopsies on deceased suicide bombers should also be routinely performed as recommended by Townsend. Indeed, the number of suicide events is not so great each year that psychological autopsies using consistent criteria could not be performed on a widespread basis. Given increasing evidence of biomarkers in suicide, psychological autopsies should be complemented by physical autopsies where possible.[80–82]
Knowing whether suicide attackers are suicidal is not simply an academic issue. In the context of growing evidence that recruitment occurs among the bereaved, those with disabilities, and even mental illness, it has clinical implications. It also has implications for prevention. If suicidality (ideation, intent, planning) plays any role in the path to becoming a suicide attacker, even for a minority of such attackers, that finding could be used at population levels to design screening programs that could potentially identify and possibly reduce the numbers of individuals who are vulnerable to recruitment. In the context of recent efforts (especially in the Arab world) to “rehabilitate” would-be terrorists, it also has implications for rehabilitation and what has been called a “soft approach” to counterterrorism.[83–87] While many of these programs were designed to “de-radicalize” and encourage renunciation of terrorist ideology and systematic efforts to evaluate them are still lacking, fighting for the “minds of suicide bombers” is a promising direction.86 There is the additional benefit that more systematic research on this phenomenon will advance the broader study of suicidal behavior itself.
References
1. Chicago Project on Security and Terrorism (CPOST). Suicide attack database. http://cpostdata.uchicago.edu/search_new.php. Accessed June 1, 2014.
2. Atran S. Genesis of suicide terrorism. Science. 2003;299:1534–1529.
3. Boaz G. Suicide Attacks in Israel. In: Countering Suicide Terrorism. Herzliya: International Policy Institute for Counter-Terrorism; 2000:134.
4. Bloom M. Dying to Kill: The Allure of Suicide Terror. New York: Columbia University Press; 2007.
5. Pape R. Dying to Win: The Strategic Logic of Suicide Terrorism. New York: Random House; 2005.
6. Pedahzur A. The Root Causes of Suicide Terrorism: The Globalization of Martyrdom. New York: Routledge; 2006:8.
7. Merari A. The readiness to kill and die: suicidal terrorism in the Middle East. In: Reich W (ed). Origins of Terrorism: Psychologies, Ideologies, Theologies, States of Mind. Washington DC: Woodrow Wilson Press; 1998:192.
8. Stern J. Terror in the Name of God. New York: Harper Collins; 2003.
9. Cronin AK. Terrorists and Suicide Attacks. Washington DC: Library of Congress; 2003.
10. Axell A, Kase H. Kamikaze: Japan’s Suicide Gods. New York: Longman; 2002.
11. Hoffman B. The logic of suicide terrorism. The Atlantic. June 1, 2003. http://www.theatlantic.com/magazine/archive/2003/06/the-logic-of-suicide-terrorism/302739/. Accessed October 1, 2014.
12. Reuters. Taliban vow suicide and “insider” attacks in new spring offensive. April 27, 2013. http://www.reuters.com/article/2013/04/27/us-afghanistan-offensive-idUSBRE93Q01Z20130427. Accessed October 1, 2014.
13. Atran S. Moral logic and growth of suicide terrorism. Washington Quarterly. 2006;29(2):127–147.
14. Brym RJ, Araj B. Suicide bombing as strategy and interaction: the case of the Second Intifada. Social Forces. 2006;84(4):1969–86.
15. Bloom M. Palestinian suicide bombing: public support, market share, and outbidding. Political Science Quarterly. 2004;119(1):61–88.
16. Crenshaw M. Explaining suicide terrorism: a review essay. Security Studies. 2007;16(1):133–162.
17. Krueger A, Maleckova J. Education, poverty and terrorism: Is there a causal connection? J Econ Perspec. 2003;17(4):119–44.
18. Abadie A. Poverty, political freedom and the roots of terrorism. Am Econ Review. 2006;96(2):50–56.
19. Piazza JA. A supply-side view of suicide terrorism: a cross-national study. J Politics. 2008;70(1):28–39.
20. Benmelech E, Berrebi C, Klor E. Economic conditions and the quality of suicide terrorism. J Politics. 2012;74(1):113–128.
21. Hafez M. Suicide Bombers in Iraq: The Strategy and Ideology of Martyrdom. Washington DC: United States Institute of Peace; 2007.
22. Moghadam A. The Globalization of Martyrdom: Al Qaeda, Salifi Jihad and the Diffusion of Suicide Attacks. Baltimore: Johns Hopkins Press; 2008.
23. Glucklich A. Dying for Heaven: Holy Pleasure and Suicide Bombers—Why the Best Qualities of Religion Are Also Its Most Dangerous. NY: HarperOne; 2009.
24. Gill P. A multi-dimensional approach to suicide bombing. Int J Confl Violence. 2007;1(2):142–159.
25. Sageman M. Understanding Terror Networks. Philadelphia, PA: University of Pennsylvania Press; 2004.
26. Atran S. Mishandling suicide terrorism. Washington Quarterly. 2004;67–90.
27. Merari A, Diamant I, Bibi A, et al. Personality characteristics of suicide bombers and organizers of suicide attacks. Terror Polit Violence. 2009;22(1):1061.
28. Pew Research Global Attitudes Project. Muslim publics share concerns about extremist groups. September 10, 2013. http://www.pewglobal.org/2013/09/10/muslim-publics-share-concerns-about-extremist-groups/. Accessed October 1, 2014.
29. Hafez MH. Manufacturing Human Bombs: The Making of Palestinian Suicide Bombers. Washington, DC: United States Institute of Peace Press; 2006.
30. Speckhard A, Akhmedova K. The new Chechen jihad: militant wahabism as a radical movement and a source of suicide terrorism in post-war Chechen society. Democracy & Security. 2006;2:1–53.
31. Fields RM, Elbedour S, Hein AF. The Palestinian suicide bomber. In Stout CE (ed). The Psychology of Terrorism: Clinical Aspects and Responses. Westport, CT: Prager Publishers; 2002:193–223.
32. Hassan N. Letter from Gaza: an arsenal of believers. New Yorker. 2001:36–41.
33. Yale Global Online. Hassan R. What motivates the suicide bomber? September 3, 2009. http://yaleglobal.yale.edu/content/what-motivates-suicide-bombers-0. Accessed October 1, 2014.
34. Hudson R. The Sociology and Psychology of Terrorism: Who Becomes a Terrorist and Why? Honolulu, HI: University Press of the Pacific; 2005.
35. Post J, Sprinzak E, Denny L. The terrorists in their own words: interviews with 35 incarcerated Middle Eastern terrorists. Terror Polit Violence. 2003;15(1):171–184.
36. Handwerk B. Female suicide bombers: dying to kill—an interview with Lisa Ling. National Geographic News. December 13, 2014. http://news.nationalgeographic.com/news/2004/12/1213_041213_tv_suicide_bombers.html. Accessed October 1, 2014.
37. Williams BG. Mullah Omar’s missiles: a field report on suicide bombers in Afghanistan. Middle East Policy Council. 2008;15(4). http://www.mepc.org/journal/middle-east-policy-archives/mullah-omars-missiles-field-report-suicide-bombers-afghanistan?print. Accessed October 1, 2014.
38. Fatah S. Why the disabled do Taliban’s deadly work. Globe and Mail. May 7, 2007. http://www.theglobeandmail.com/news/world/why-the-disabled-do-talibans-deadly-work/article18138707/ Accessed Oct. 1, 2014
39. Nelson SS. Disabled often carry out Afghan suicide missions. National Public Radio, Morning Edition, October 15, 2007.http://www.npr.org/templates/story/story.php?storyId=15276485. Accessed October 1, 2014.
40. Brym RJ, Araj B. Are suicide bombers suicidal? Stud Confl Terror. 2012;35(6):432–443.
41. Merari A. Driven to Death: Psychological and Social Aspects of Suicide Terrorism. Oxford, UK: Oxford University Press; 2010.
42. Speckhard, A. Akhmedova K. Black widows: the Chechen female suicide terrorists. In: Schweitzer Y (ed). Female Suicide Bombers: Dying for Equality? Tel Aviv: Jafee Center for Strategic Studies; 2006:63–80.
43. Lankford A. The Myth of Martyrdom: What Really Drives Suicide Bombers Rampage Shooters and Other Self-Destructive Killers? New York: Palgrave Macmillan; 2013.
44. Townsend E. Suicide terrorists: are they suicidal? Suicide Life-Threat. 2007;37(1):35–49.
45. Nock MK, Borges G, Bromet EJ, et al. Cross–national prevalence and risk factors for suicidal ideation, plans and attempt. Br J Psychiatry. 2008;192:98–105.
46. Rogers MB, Lowenthal KM, Lewis CA, et al. The role of religious fundamentalism in terrorist violence: a social psychological analysis. Int. Rev Psychiatry. 2007;19(3):253–262.
47. Pedersen NL, Fiske A. Genetic influences on suicide and nonfatal suicidal behavior: twin study findings. Eur Psychiatry. 2010;25:264–267.
48. Harris EC, Barraclough B. Suicide as an outcome for mental disorders: a meta-analysis. Br J Psychiatry.1977;170:205–228.
49. Mann JJ, Arango VA, Avervole S, et al. Candidate endophenotypes for genetic studies of suicidal behavior. Biol Psychiatry. 2009;65(7):556–563.
50. Brent DA, Melhem V. Familial transmission of suicidal behavior. Psychiatr Clin N Am. 2008;31(2):157–577.
51. Tondo L, Balldesarini RJ. Can suicidality be prevented? Psychiatric Times. 2011;28(2).
52. Tondo L, Balldesarini RJ. Long-term lithium treatment in the prevention of suicidal behavior in bipolar disorder patients. Epidemiol Psychiatr Soc. 2009;18(3):179–83.
53. Balldesarini RJ, Tondo L. Lithium and suicidal risk. Bipolar Disord. 2008;10(1):114–5.
54. Meltzer HY, Okayli G. Reduction of suicidality during clozapine treatment of neuroleptic-resistant schizophrenia: impact on risk-benefit assessment. Am J Psychiatry. 1995;152:183–190.
55. Berko A. The Path to Paradise: The Inner World of Suicide Bombers and their Dispatchers. Potomac Books; 2009:1.
56. Okasha A, Okasha T. Suicide and Islam. In: Wasserman D, Wasserman C (eds). Suicidology and Suicide Prevention: A Global Perspective. Oxford: Oxford University Press; 2009:50–55.
57. Bodner E, Ben-Artzi E, Kaplan Z. Soldiers who kill themselves: the contribution of dispositional and situational factors. Arch Suicide Res. 2006;10:29–43.
58. Oquendo M, Galfalvy H, Russo S, et al. Prospective study of clinical predictors of suicidal acts after a major depressive episode in patients with major depressive disorder or bipolar disorder. Am J Psychiatry. 2004;161:1433–1441.
59. Smith A, Witte TK, Teal N, et al. Revisiting impulsivity in suicide. Behav Sci Law. 2008;26(6):779–797.
60. Pritchard C. Suicide—The Ultimate Rejection? A Psychological Study. Buckingham, UK: Open University Press, 1996.
61. Dervic K, Oquendo MA, Grunebaum MF, et al. Religious affiliation and suicide attempt. Am J Psychiatry. 2004;161:2303–2308.
62. Nonnemaker JM, McNeely CA, Blum RW. Public and private domains of religiosity and adolescent health risk behaviors: evidence from the National Longitudinal Study of Adolescent Health. Soc Sci Med. 2003;57(11):2049–2054.
63. Bughra D. Commentary: religion, religious attitudes and suicide. Int J Epidemiol. 2010;9(6):1496–98.
64. Moghadamnia AA, Abdollahi M. An epidemiological study of poisoning in northern Islamic Republic of Iran. E. Mediterranean Health J. 2002;8:88–94.
65. Al-Jahdali H, Al-Johani A, Al-Hakawi A, et al. Pattern and risk factors for intentional drug overdose in Saudi Arabia. Can J Psychiatry. 2004;49;331–334.
66. Wasserman D, Cheng Q, Jiang GX. Global suicide rates among young people aged 15–19. World Psychiatry. 2005;4(2):114–120.
67. Pritchard C, Amanullah S. An analysis of suicide and undetermined deaths in 17 predominantly Islamic countries contrasted with the UK. Psychol Med. 2007;37:421–430.
68. Zai CC, de Luca V, Straus J. Genetic factors and suicidal behavior. In: Dwivedi (ed.) The Neurobiological Basis of Suicide. CRC Press; 2012. http://www.ncbi.nlm.nih.gov/books/NBK107191/. Accessed October 1, 2014.
69. Roy A, Segal NL. Suicidal behavior in twins: a replication. J Affect Dis. 2001;66(1):71–74.
70. Brent D, Mann JJ. Family genetic studies, suicide, and suicidal behavior. Am J Med Genet. 2005;133C(1):13–24.
71. Labonte B, Suderman M, Maussion G, et al. Genome-wide methylation changes in the brains of suicide completers. Am J Psychiatry. 2013;170:511–520.
72. Global Terrorism Database. National Consortium for the Study of Terrorism and Responses to Terrorism (START). 2012. http://www.start.umd.edu/gtd. Accessed October 1, 2014.
73. National Security Studies Center of the University of Haifa, Israel. Suicide Terrorism Database. http://nssc.haifa.ac.il/index.php/en/. Accessed October 1, 2014.
74. Terrorism Resesarch & Analysis Consortium. Suicide Terrorism Database—Flinders University, Australia. Available at: http://www.trackingterrorism.org/resource/suicide-terrorist-database-flinders-university-australia. Accessed October 1, 2014.
75. Sageman M. Fighting the right war. National Defense University Joint Operations Symposium. March 16–17, 2006. http://www.artisresearch.com/articles/Sageman_Fighting_the_Right_War.pdf. Accessed October 1, 2014.
76. Sheehan DV, Lecrubier Y, Sheehan KH, et al. The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. 1998;59(20 Suppl): 22–33
77. Coric V, Stock EG, Pulz J. Sheehan-Suicidality Tracking Scale (S-STS): preliminary results from a multicenter clinical trial in generalized anxiety disorder. Psychiatry (Edgmont). 2009;6(1):26–31.
78. Preti A, Sheehan DV, Coric V et al. Sheehan Suicidality Tracking Scale (S-STS): reliability, convergent and discriminative validity in young Italian adults. Compr Psychiatry. 2013;54(7):842–849.
79. Sheehan, IS, Sheehan DV. Homicidality Scale (S-HTS). http://professorsheehan.com/category/homicidality-scale/. Accessed October 1, 2014.
80. Le-Niculescu H, Levey DF, Ayalew M, et al. Discovery and validation of blood biomarkers for suicidality. Molecular Psychiatry. 2013;18(12):1249–1264.
81. Pandey GN, Pandey SC, Dwivedi Y, et al. Platelet serotonin-2A receptors: a potential biological marker for suicidal behavior. Am. J. Psychiatry. 1995;152(6):850–855.
82. Pan LA, Hassel S, Segreti AM, et al. Differential patterns of activity and functional connectivity in emotion processing neural circuitry to angry and happy faces in adolescents with and without suicide attempt. Psychol Med 2013;43(10):2129–2142.
83. Perspectives on Terrorism. Stracke N. Arab prisons: a place for dialogue and reform. 2007. http://terrorismanalysts.com/pt/index.php/pot/article/view/15/html. Accessed October 1, 2014.
84. Boucek C. Counter-terrorism from within. Assessing Saudi Arabia’s religious rehabilitation and disengagement programme. RUSI J. 2008;153(6):60–65.
85. Horgan J, Braddock K. Rehabilitating the terrorists? challenges in assessing the effectiveness of de-radicalization programs. Terror Polit Violence. 2010;22:267–291.
86. Angeli A, Gunaratna R. Terrorist Rehabilitation: The U.S. Experience in Iraq. Boca Raton, FL: Taylor and Francis; 2012.
87. Bell S. Reason to live: in Southeast Asia, fighting terror includes fighting for the minds of suicide bombers. National Post (Canada). 2006 Feb 25. http://www2.canada.com/national/nationalpost/news/cnspolitics/story.html?id=1ac3ee9e-4c7f-450f-9e21-f0dc94e0dd01&p=1.