
by Masaru Nakamura, MD, PhD, and Takahiko Nagamine, MD, PhD
Dr. Nakamura is with the Department of Psychiatric Internal Medicine, Kosekai-Kusatsu Hospital in Hiroshima, Japan. Dr. Nagamine is with the Department of Psychiatric Internal Medicine, Sunlight Brain Research Center in Yamaguchi, Japan.
Funding: No funding was provided for this study.
Disclosures: The authors have no conflicts of interest relevant to the content of this article.
Abstract: Atypical antipsychotics, used to treat patients with schizophrenia, focus on dopamine-2 (D2) plus serotonin-2A (5-HT2A) receptor antagonism and currently carry different degrees of certain adverse effects. Brexpiprazole is a new serotonin–dopamine receptor modulator that acts as a partial agonist at the 5-HT1A and D2 receptors. In patients who were either introduced to brexpiprazole because of nonadherence to traditional medications or were switched from apripiprazole, olanzapine, or paliperidone, the impact of brexpiprazole on different parameters was evaluated. Ultimately, it was found that brexpiprazol treatment displayed a low propensity to influence metabolic parameters (lipids and glucose) and minimal impact on prolactin levels. Further prospective and longer follow-up studies involving larger groups of subjects are required.
Keywords: Antipsychotics, aripiprazole, brexpiprazole, metabolism, olanzapine, paliperidone, prolactin
Innov Clin Neurosci. 2019;16(9–10):30–32
Atypical antipsychotics, currently used to treat patients with schizophrenia, focus on dopamine-2 (D2) plus serotonin-2A (5-HT2A) receptor antagonism and carry different degrees of certain adverse effects, such as metabolic syndrome and hyperprolactinemia.1,2 Changes in lipid and glucose might arise independently of weight gain during treatment with atypical antipsychotics, most of which inhibit a range of other receptors (e.g., serotonin-2C [5-HT2C], histamine-H1 (H1), adrenergic-alpha-1A (alpha-1A), and muscarinic-3 (M3) receptors].3 We have reported previously on the relationships between the potency of 5-HT2C blockade and hypertriglyceridemia and the potency of M3 blockade and glucose intolerance in patients switched from olanzapine to clozapine or asenapine.4 Hyperprolactinemia is considered to be primarily a result of D2 receptor blockade, which causes a loss in the dopaminergic inhibitory effect on prolactin secretion. Although most of the antipsychotic drugs induce elevations in prolactin levels, depending on the D2 receptor occupancy and the antagonistic properties of the antipsychotics, the partial dopamine agonist aripiprazole instead decreases the prolactin level.2
Brexpiprazole is a new serotonin–dopamine receptor modulator that acts as a partial agonist at the 5-HT1A and D2 receptors with less intrinsic activity than aripiprazole and as an antagonist at the 5-HT2A and alpha-1A receptors, all with subnanomolar potency.5 To investigate the effects of brexpiprazole on metabolic parameters and prolactin levels, inpatients treated with brexpiprazole who discontinued other antipsychotics or were switched from olanzapine (having the strongest metabolic effect and an intermediate prolactin elevation effect), paliperidone (having an intermediate metabolic effect and the strongest prolactin elevation effect), or aripiprazole (having the weakest metabolic effect and a prolactin reduction effect) were recruited. The ethics committee of Kusatsu Hospital in Hiroshima, Japan approved this study. Informed consent was received from all study participants.
Subjects and Methods
Patients being treated with antipsychotics other than brexpiprazole concomitantly during the study period were excluded. A total of 40 subjects was included in this study: 15 subjects (5 male and 10 female subjects with a mean age of 48 years) were introduced to brexpiprazole due to nonadherence; 14 subjects (8 male and 6 female subjects with a mean age of 44 years) were switched from aripiprazole; five subjects (2 male and 3 female subjects with a mean age of 47 years) were switched from olanzapine; and six subjects (2 male and 4 female subjects with a mean age of 45 years) were switched from paliperidone. Body weight (BW), fasting plasma glucose (FBS), insulin (IRI), triglyceride (TG), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), and prolactin (PRL) levels were measured at baseline and one month after brexpiprazole treatment. Within each subgroup, the Wilcoxon signed-rank test was used to compare these levels, and results were considered statistically significant at p<0.05. We assumed that the closed-ward and short-term setting would minimize interindividual differences in energy intake and expenditure and internal intervention.
Results
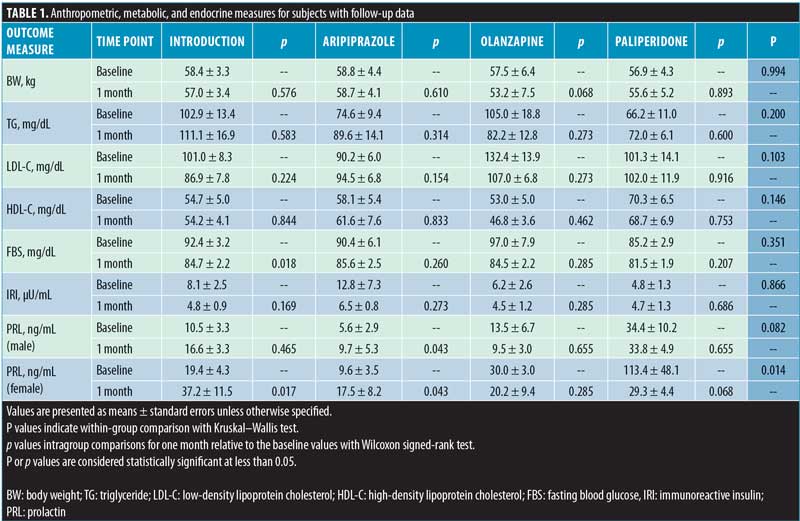
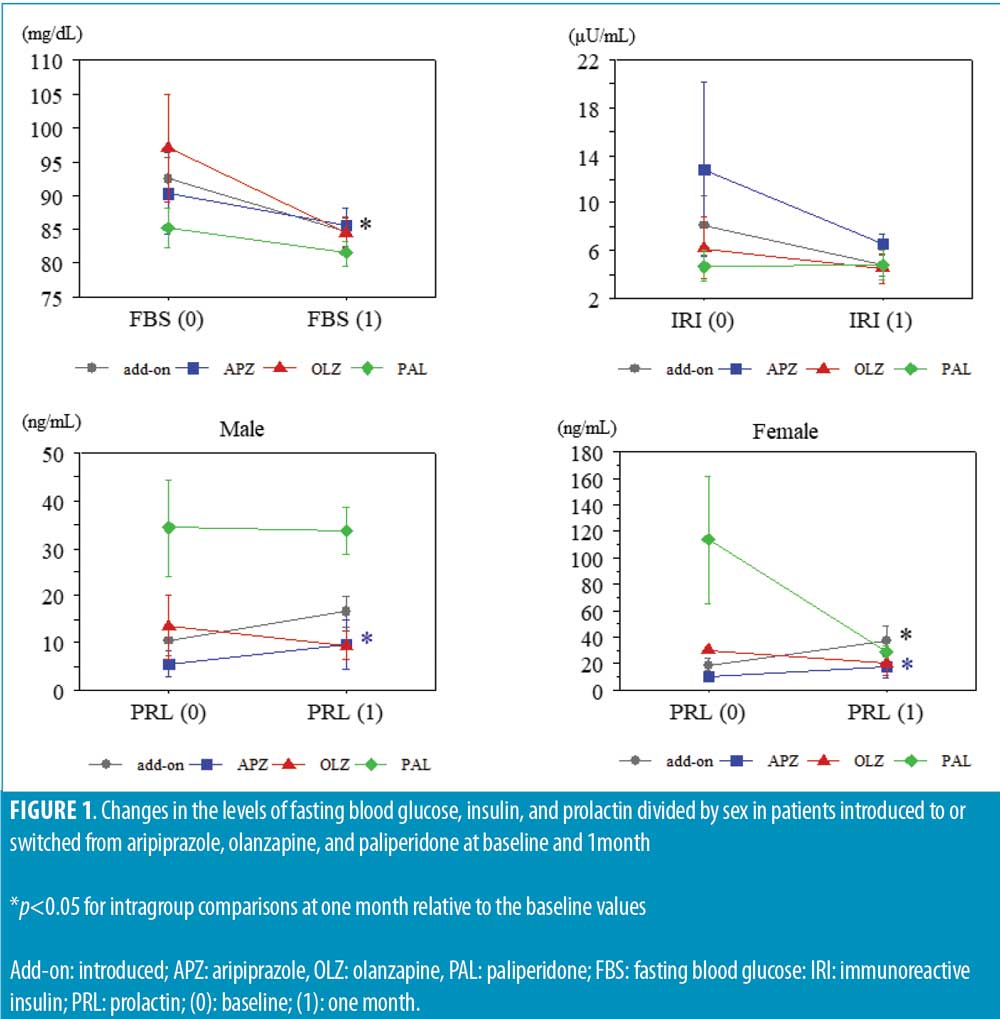
The BW and TG levels tended to decrease in subjects switched from olanzapine to brexpiprazole. The LDL-C levels tended to decrease in subjects switched from olanzapine to brexpiprazole and in subjects who were introduced to brexpiprazole, and tended to increase in subjects switched from aripiprazole to brexpiprazole, whereas HDL-C levels remained unchanged in all groups. The FBS levels significantly decreased in subjects who were introduced to brexpiprazole and decreased to a lesser degree in all other groups. The IRI levels tended to decrease and reached the same lower levels in all subjects. The PRL levels significantly increased in male patients switched from aripiprazole to brexpiprazole; conversely increased in female patients who were introduced to brexpiprazole and switched from aripiprazole to brexpiprazole, and tended to decrease in female subjects switched from paliperidone or olanzapine to brexpiprazole (Table 1 and Figure 1).
Discussion
The strength of this study was that brexpiprazol treatment displayed a low propensity to influence metabolic parameters (i.e., lipids and glucose) and had a minimal impact on prolactin level.
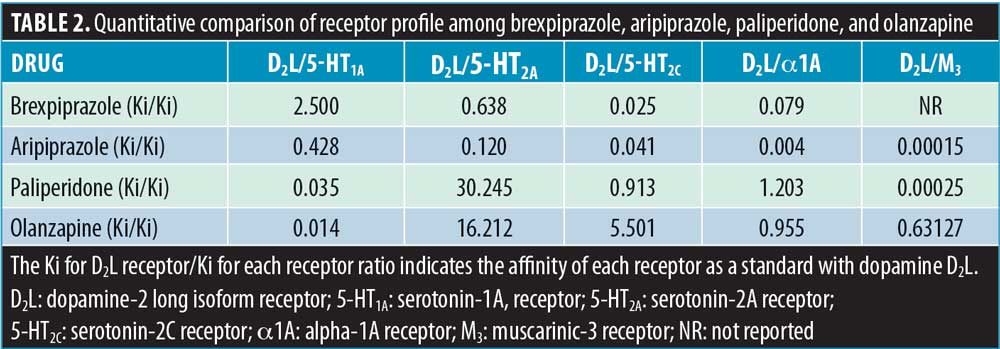
Among in-vitro receptor-binding profiles,6 the antagonism of 5-HT2C, 5-HT2A, alpha-1A, and M3 receptors and the agonism of 5-HT1A receptors are thought to play major roles in each metabolic change. The potency of 5-HT2C receptor blockade of olanzapine, which reduces central sympathetic outflow and elicits substantial reductions in the cost of energy, exceeds that of brexpiprazol. The potency of muscarinic (M3) receptor blockade, which controls cholinergic-stimulated pancreatic insulin secretion, is expressed as follows: olanzapine > paliperidone > aripiprazole/brexpiprazol. Moreover, the potency of 5-HT2A and alpha-1A receptor blockade of paliperidone and olanzapine is much stronger than that of aripiprazole and brexpiprazol, while the potency of 5-HT1A receptor stimulation is the highest in brexpiprazol (Table 2). Guenette et al7 reported that treatment with prazosin, a selective alpha-1 antagonist, and MDL100907, a selective 5-HT2A antagonist, resulted in significant decreases in both insulin and C-peptide secretion. Gilles et al8 reported that the selective 5-HT2 antagonist, ketanserin, impaired insulin sensitivity and that this effect was possibly mediated by the suppression of 5-HT2A receptor–mediated glucose uptake in the skeletal muscle. Sugimoto et al9 suggested that buspirone, a 5-HT1A receptor agonist, reduces stress-induced hyperglycemia by facilitating insulin release. These studies support the theory that brexpiprazol treatment directly reduces insulin resistance.
A key issue facing D2 partial agonism is the need to determine an optimal level of intrinsic activity that would lead to a desirable stabilization of dopaminergic transmission. Too high of a level of D2 intrinsic activity leads to a lack of robust clinical activity as well as adverse effects related to increased D2 receptor tonus (e.g., nausea, vomiting, insomnia, and motor effects, such as hyperkinesia and restlessness), whereas excessive D2 antagonist activity results in an increased risk for extrapyramidal symptoms and increased prolactin secretion.5 Intrinsically, brexpiprazol is a more potent dopamine antagonist than aripiprazole, though less potent than a pure antagonist;10 the pharmacological profile of brexpiprazol on prolactin levels was demonstrated in a clinical setting.
Limitations. Retrospective design, small sample size, and short observation period limit our findings. However, the exploration of receptor-binding profiles might be useful to estimate the favorable metabolic and prolactin changes in patients treated with atypical antipsychotics including a serotonin dopamine receptor modulator. Further prospective and longer follow-up studies in larger groups of patients are required to confirm our findings.
Conclusion
Brexpiprazol treatment displayed a low propensity to influence metabolic parameters and minimal impact on prolactin levels, which was estimated from receptor-binging profiles among atypical antipsychotics.
References
- Meyer JM, Davis VG, Goff DC, et al. Change in metabolic syndrome parameters with antipsychotic treatment in the CATIE Schizophrenia Trial: prospective data from phase 1. Schizophr Res. 2008;101(1–3):273–286.
- Peuskens J, Pani L, Detraux J, et al. The effects of novel and newly approved antipsychotics on serum prolactin levels: a comprehensive review. CNS Drugs. 2014;28(5):421–453.
- Montastruc F, Palmaro A, Bagheri H, et al. Role of serotonin 5-HT2C and histamine H1 receptors in antipsychotic-induced diabetes: A pharmacoepidemiological-pharmacodynamic study in VigiBase. Eur Neuropsychopharmacol. 2015;25(10):1556–1565.
- Nakamura M, Nagamine T. Metabolic changes in patients with schizophrenia switched from olanzapine to asenapine or clozapine. Innov Clin Neurosci. 2018;15
(7–8):11–12. - Maeda K, Sugino H, Akazawa H, et al. Brexpiprazole I: in vitro and in vivo characterization of a novel serotonin-dopamine activity modulator. J Pharmacol Exp Ther. 2014;350(3):589–604.
- Shahid M, Walker GB, Zorn SH, Wong EH. Asenapine: a novel psychopharmacologic agent with a unique human receptor signature. J Psychopharmacol. 2009;23(1):65–73.
- Guenette MD, Giacca A, Hahn M, et al. Atypical antipsychotics and effects of adrenergic and serotonergic receptor binding on insulin secretion in-vivo: an animal model. Schizophr Res. 2013;146(1–3):162–169.
- Gilles M, Wilke A, Kopf D, et al. Antagonism of the serotonin (5-HT)-2 receptor and insulin sensitivity: implications for atypical antipsychotics. Psychosom Med. 2005;67(5):748–751.
- Sugimoto Y, Takashima N, Noma T et al. Inhibitory effects of the 5-HT1A receptor agonist buspirone on stress-induced hyperglycemia in mice: involvement of insulin and a buspirone metabolite, 1-(2-Pyrimidinyl)piperazine (1-PP). Biol Pharm Bull. 2005;28(4):733–735.
- Frampton JE. Brexpiprazole: a review in schizophrenia. Drugs. 2019;79(2):189–200.