
 by Chiranjir Narine, MD; Jennifer Weller, PhD; and Kathleen Mathieson, PhD, CIP
by Chiranjir Narine, MD; Jennifer Weller, PhD; and Kathleen Mathieson, PhD, CIP
Dr. Narine is the Medical Director of Valleywise Behavioral Health/District Medical Group in Phoenix, Arizona. Dr. Weller is the Research Director in the Child Psychiatry Department at Valleywise Behavioral Health/District Medical Group. Dr. Mathieson is an Associate Professor with the Doctor of Health Sciences Program at A.T. Still University in Mesa, Arizona.
FUNDING: No funding was provided for this study.
DISCLOSURES: The author has no conflict of interest relevant to the content of this article.
ABSTRACT: Objective. We sought to determine the frequency, reasons for, and factors associated with energy drink consumption in adolescents with or without attention deficit hyperactivity disorder (ADHD).
Design. Anonymous surveys were completed by 115 adolescents and their parents prior to appointments at two separate outpatient clinics (pediatric and psychiatric) over a three-month period. Trained staff provided surveys to be completed by adolescents and their parents on a voluntary basis, and all data was self-reported. Care was given to ensure adolescents and their parents completed surveys independently from each other.
Results. A total of 114 adolescent surveys and 100 parent surveys were included in analysis. There was a statistically significant association between parent and adolescent consumption of energy drinks. The mean number of energy drinks consumed in the past month was lower among adolescents than among parents. The most common reason among all respondents for energy drink consumption was to promote wakefulness.
Conclusion. This survey found that adolescents with parents who consumed energy drinks were more likely to drink energy drinks themselves. Trends indicate that consumption of energy drinks is increasing in the adolescent population, with potential for serious adverse events resulting from high caffeine content, warranting the need for public health awareness.
Keywords: Energy drink, ADHD, attention deficit hyperactivity disorder, child and adolescent psychiatry, pediatric psychiatry, sports drinks, Red Bull, Monster Energy, caffeine, stimulants, coffee, Starbucks, 5 hour energy
Innov Clin Neurosci. 2021;18(4–6):xx–xx
Energy drinks are beverages containing stimulants, such as caffeine and certain herbal extracts, with the stated goal of enhancing physical and mental endurance.1 Over the last few decades, the popularity of energy drinks has risen around the world with reported regular consumption by 28 percent of youths 12 to 14 years old, 31 percent of youths 12 to 17 years old, and 34 percent of young adults.2, 9
Energy drinks were first introduced in the United States in 1949 under the label “Dr. Enuf,” a carbonated beverage fortified with B vitamins. By the 1960s, energy drinks were available in Asia and Europe. In 1962, Lipovitan D became available (an energy drink that continues to dominate the Japanese market).3 In 1987, Red Bull was founded and marketed in Austria; it did not become successful until introduction to the US in 1997. Since then, the market has grown exponentially, with over 300 different brands currently marketed and sold in the United States.1
Globally, energy drinks have exhibited strong sales. In 2008, this sector comprised 42.4 percent of the overall “functional drinks” market, with a total revenue of $11.8 billion (compared to $5.1 billion in 2003).4 Initially, athletes were the primary target for energy drinks but recent research shows that adolescents, young adults (ages 16–35), and young female adolescents/adults in particular have become the primary groups that are now targeted.5 The global energy drink market was projected to hit over $37 billion in 2014,4 but instead hit $49.9 billion. Despite the popularity of energy drinks in the US, from 2007 to 2009 the energy drink market remained a flat 15 percent of individuals aged 18 and older consuming energy drinks. This situation caused manufacturers to target women, herb and vitamin enthusiasts, the affluent, and the youth to increase sales. The sales of energy drinks making a “low, no, or reduced calorie” claim increased from 6 percent to 11 percent between 2004 and 2008. This competition led soft drink manufacturers to include energy drinks in their beverage market.6
Most energy drinks contain one or more of the following: caffeine, guarana, taurine, ginseng, sugars, and B vitamins (i.e. riboflavin, pyridoxine) in varying amounts. Caffeine is rarely listed as an official ingredient, and when caffeine content is stated the amount is often inaccurate, due to the additional caffeine content from guarana not typically being included.17 The US Food and Drug Administration (FDA) regulates the amount of caffeine in cola beverages (≤65mg per 12oz) but does not regulate the amount of caffeine in energy drinks and cold coffee beverages, because caffeine is generally recognized by the FDA as safe for consumption.2, 17
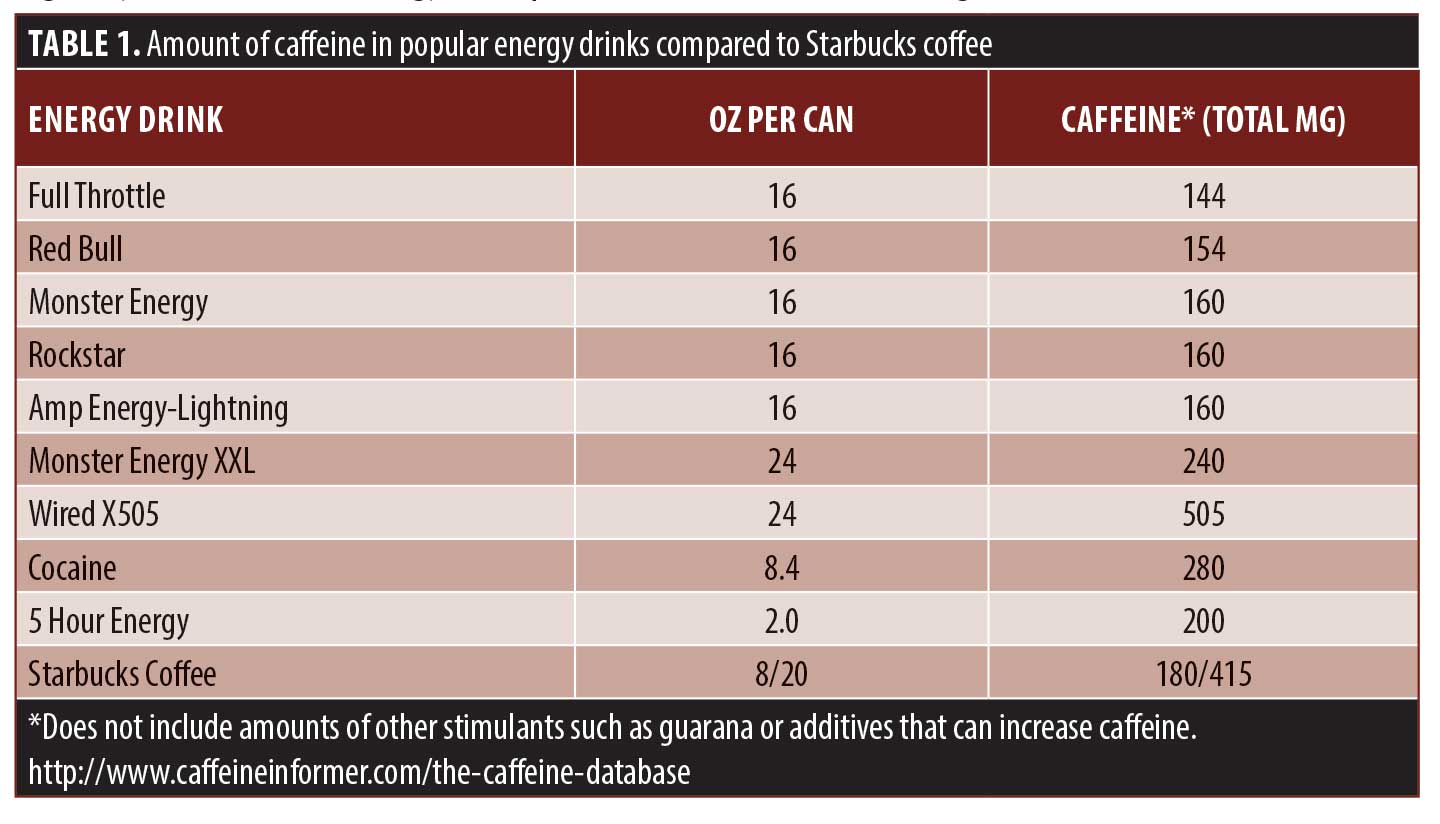
A 6.5-oz cup of caffeinated coffee contains 80 to 120mg of caffeine, and an 8-oz cup of caffeinated tea contains approximately 50mg of caffeine. A 12-oz cola beverage, by law, cannot contain more than 65mg of caffeine. Even carbonated fountain sodas sold at fast food establishments and at gas stations contain less than 49mg of caffeine per 16-oz serving. The amount of caffeine in 16-oz energy drinks can range from 154 to 280mg (the equivalent of 2–3 cups of caffeinated coffee), while some energy drinks contain 500mg or more in a single can.7 The only recommendation in the US for limitations of caffeine consumption comes from the American Dietetic Association, which recommends that women of reproductive age and children should not exceed 300mg of caffeine per day (2–3 cups of coffee).
Several adverse health conditions have been linked to energy drink consumption, including anxiety, headache, fatigue,2 neuropathy,12 seizures, liver damage, kidney failure, respiratory disorders, agitation, psychosis,13 atrial and ventricular fibrillation, and even cardiac arrest.14 Table 1 shows the range of caffeine present in popular energy drinks compared to one cup of Starbucks coffee.
Energy drinks also often contain ingredients that enhance or mimic the effects of caffeine. Guarana is Paullinia cupana a South American plant, commonly used in energy drinks. It contains guaranine which is chemically identical to caffeine. One gram of guarana is equivalent to 40mg of caffeine.8 Energy drinks that list their caffeine content usually do not take into account the guarana content.
Consumption of energy drinks by children, adolescents, and young adults. In the US, caffeine intake among adolescents averages 60 to 70mg per day and ranges up to 800mg per day.2 In addition, 28 percent of 12 to 14 year olds, 31 percent of 12 to 17 year olds, and 34 percent of 18 to 24 year olds reported regularly consuming energy drinks.9 Among 10 to 13 year olds, 31 percent of girls and 50 percent of boys have tried energy drinks. Five percent of girls and 23 percent of boys reported consuming them regularly (1 can/week).2 A survey of 496 college students found that 51 percent of participants regularly consumed one energy drink per month,10 while the majority reported consuming energy drinks several times per week. A 2014 focus group study of 240 adolescents aged 12 to 1511 years identified three general reasons for consuming energy drinks. These included “enjoyment”, “function” and “social.” Enjoyment refers to consuming energy drinks for the taste or flavor. Function is described as providing an energy boost when playing sports or when a person feels tired. Social reasons were the most common response, and related to spending time with friends (e.g. drinking energy drinks during a social event).
Although the frequency of soft drink and sweetened beverage consumption within the general adolescent population has been evaluated, few studies have examined energy drinks and the factors associated with their consumption in subgroups of the youth population. Literature searches failed to identify any studies that focused on energy drink usage among individuals diagnosed with attention deficit hyperactivity disorder (ADHD). With the reported rates of adults and youths consuming energy drinks to improve and enhance focus, we expected to see a higher rate of consumption within the ADHD subgroup compared to the non-ADHD population. Given rapidly increasing sales and the popularity of energy drinks among youth, the question of what other uses beyond taste, function, and social reasons might exist in adolescents with ADHD and their parents arose. To address this gap in the literature, and to inform public health efforts regarding consumption, the current study used data from a population-based survey to assess patterns of energy drink consumption among adolescents with or without the diagnosis of ADHD, and to examine associations with parent consumption of energy drinks. These factors were selected based on their potential for modification and to improve overall health if addressed as part of interventions focusing on healthy consumption of energy drinks within the adolescent population.
Methods
Study design. A population-based survey was designed to gather information about frequency of energy drink consumption, reasons for consuming energy drinks, most popular brands of energy drinks consumed, and factors associated with energy drink use in an adolescent population with or without ADHD and their parents.
Participants. Anonymous surveys were completed by 114 adolescents and 100 of their parents prior to appointments at two separate outpatient clinics (pediatric and psychiatric) over a three-month period. Respondents included adolescents from a predominantly low socioeconomic background in the greater Phoenix, Arizona, area. Both outpatient clinics serve a majority of patients who are uninsured or under-insured. Consideration was given to minimum enrollment size, age of participants, confidentiality, and protection of patient medical data. Approval for the study was granted by the Maricopa Integrated Health System Institutional Review Board (IRB). A waiver of informed consent/assent was granted by the Institutional Review Board.
Procedure. Trained staff provided surveys to adolescents and their parents to complete on a voluntary basis, and all data was self-reported. Care was given to ensure adolescents and their parents completed surveys independently from each other. A cover letter explaining the study purpose and procedures was included with the survey. The survey was provided in English or Spanish, based on the preference of the respondent. Parent and adolescent surveys were linked with a unique identification code; no other identifying information was required.
The adolescent version of the survey included age and sex demographics, with nine items asking about the frequency of energy drink intake, favorite brands of energy drinks, age of first use of energy drinks, and age of first consumption of multiple energy drinks per day. Location of consumption of energy drinks and reasons for consuming these beverages were also assessed. The parent version of the survey included age, sex, and 12 items similar to the adolescent version of the survey. Additional items included whether there was a diagnosis of ADHD in the parent or the adolescent and parent knowledge of their adolescent’s use of energy drinks.
Means, standard deviations, and minimum and maximum values were calculated for continuous variables. Frequencies and percentages were calculated for categorical variables. Chi-square tests were used to evaluate the association between energy drink consumption and ADHD status and the association between parent and adolescent consumption of energy drinks. The alpha value was set to 0.05, two-tailed. A power analysis indicated that 90 subjects would provide 80 percent power to detect a medium effect size of 0.30 in chi-square analyses evaluating the association between parent and adolescent energy drink consumption and between ADHD status and energy drink consumption among parents and youth.
Results
A total of 115 adolescents submitted the survey. One adolescent survey was blank, and was therefore excluded from analyses. A total of 115 parents submitted the survey. Eleven parent surveys were blank, and four participants who identified themselves as parents indicated that they were not a parent or guardian of the adolescent accompanying them. These 15 surveys were excluded, leaving a total of 100 parent surveys for analysis. Adults who did not respond to the item asking confirmation of being a parent or a guardian (n=37) were assumed to be a parent or guardian and were included in analyses.
Descriptive statistics for parents and adolescents are presented in Table 2. The mean age of adolescents completing the survey was 15±1.7 years and mean age of parents was 43±7.5 years. The majority of youth and parent respondents were female (60% and 72%, respectively). Five parents reported that they were diagnosed with ADHD, and 11 parents reported that their child had been diagnosed with ADHD. Twenty-five percent of adolescents and 16 percent of parents reported consuming energy drinks. Energy drink consumption was not associated with ADHD status among parents [Χ2 (1, N=69) = 0.058, p=.809] or among adolescents [Χ2 (1, N=72) = 1.67, p=.197].
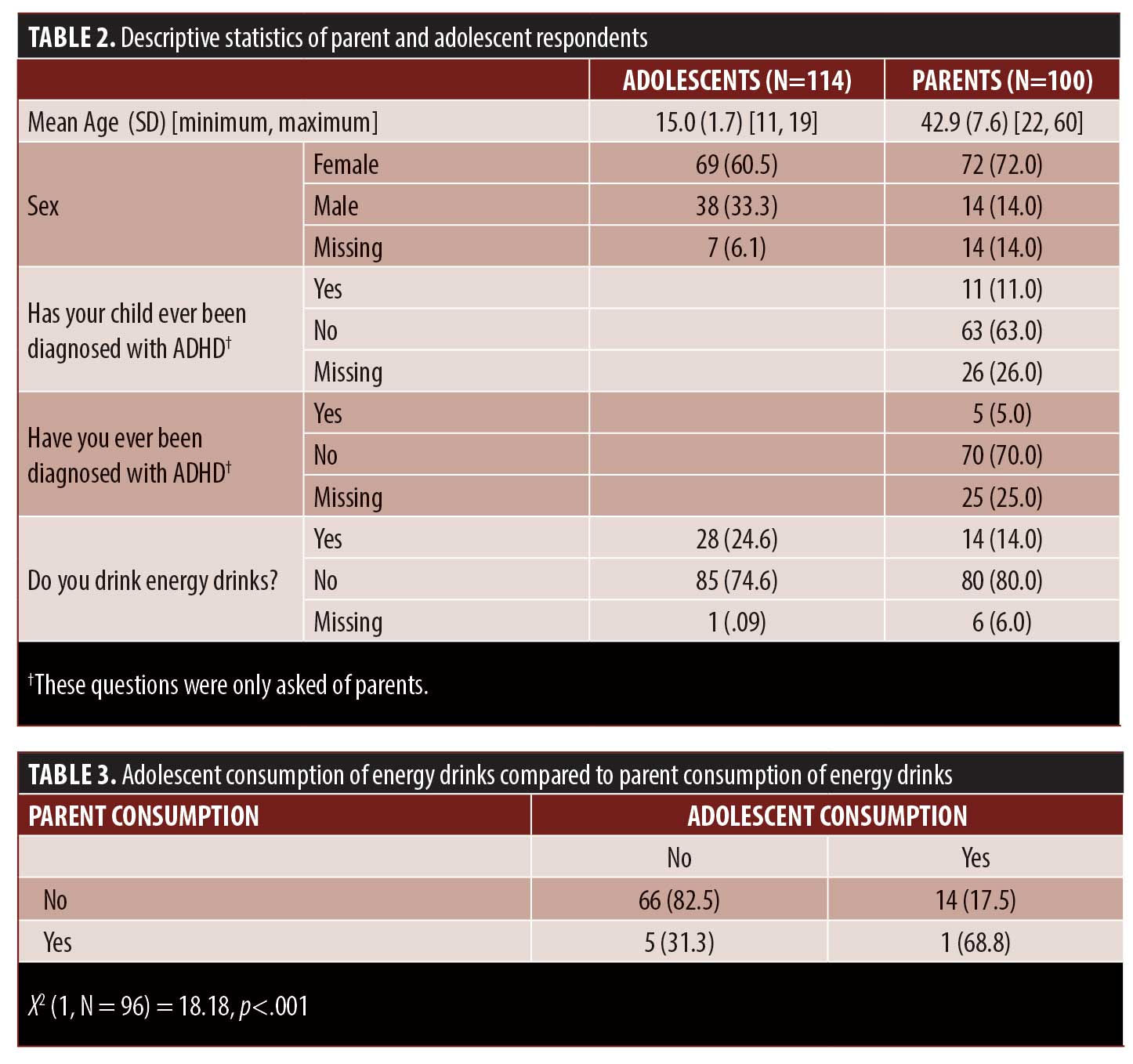
There was a statistically significant association between parent and adolescent consumption of energy drinks (Table 3). Sixty-four percent of parents who consumed energy drinks had adolescents who also consumed energy drinks. In contrast, only 18 percent of parents who did not consume energy drinks had adolescents who consumed energy drinks. Among adolescents who reported that they consumed energy drinks, 76 percent of their parents were aware of their child’s energy drink consumption. On average, adolescents who reported consumption of energy drinks endorsed drinking approximately one (0.96±1.9) energy drink in the past week. The mean number of energy drinks consumed in the past month was lower among adolescents (2.9±2.9 drinks) than among parents (10.4±12.1 drinks). Of the 14 parents who reported consuming energy drinks, only five (36%) reported consuming them with their child.
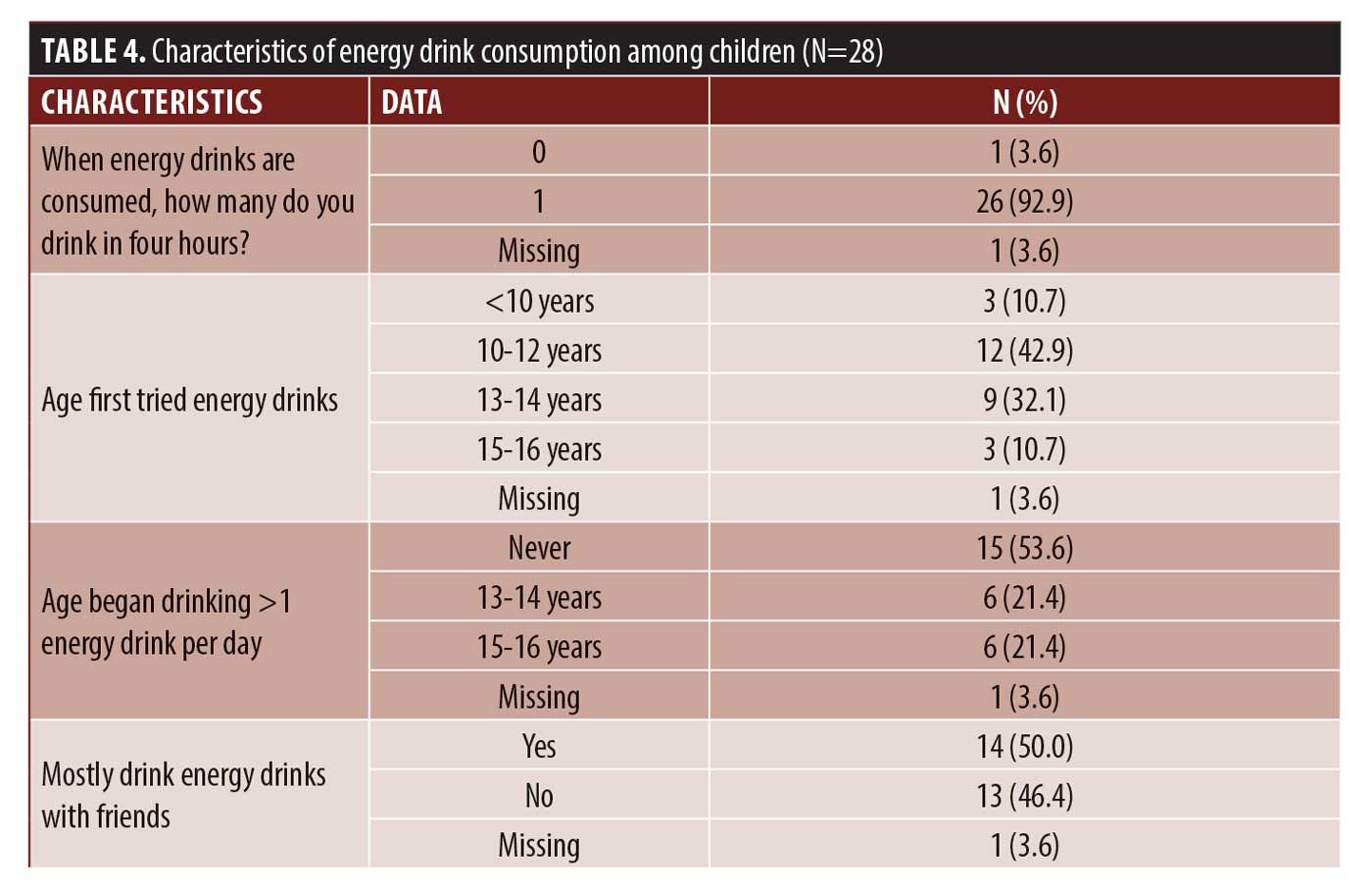
Of the 28 youths who reported consuming energy drinks, none reported drinking more than one energy drink in a four-hour period. Forty-three percent of adolescents reported that they first tried energy drinks between the ages of 10 and 12 years, and 32 percent reported that they first tried energy drinks between the ages of 13 and 14 years. Results also showed that 11 percent of adolescents reported that they first tried energy drinks prior to the age of 10 years. Twelve out of 28 adolescents who reported consuming energy drinks (43%) reported that they consumed more than one beverage per day, and these 12 adolescents all reported that they began consuming more than one energy drink per day after the age of 13 years. Half of the 28 children who reported daily consumption of energy drinks reported that they mainly consumed them with friends (Table 4).
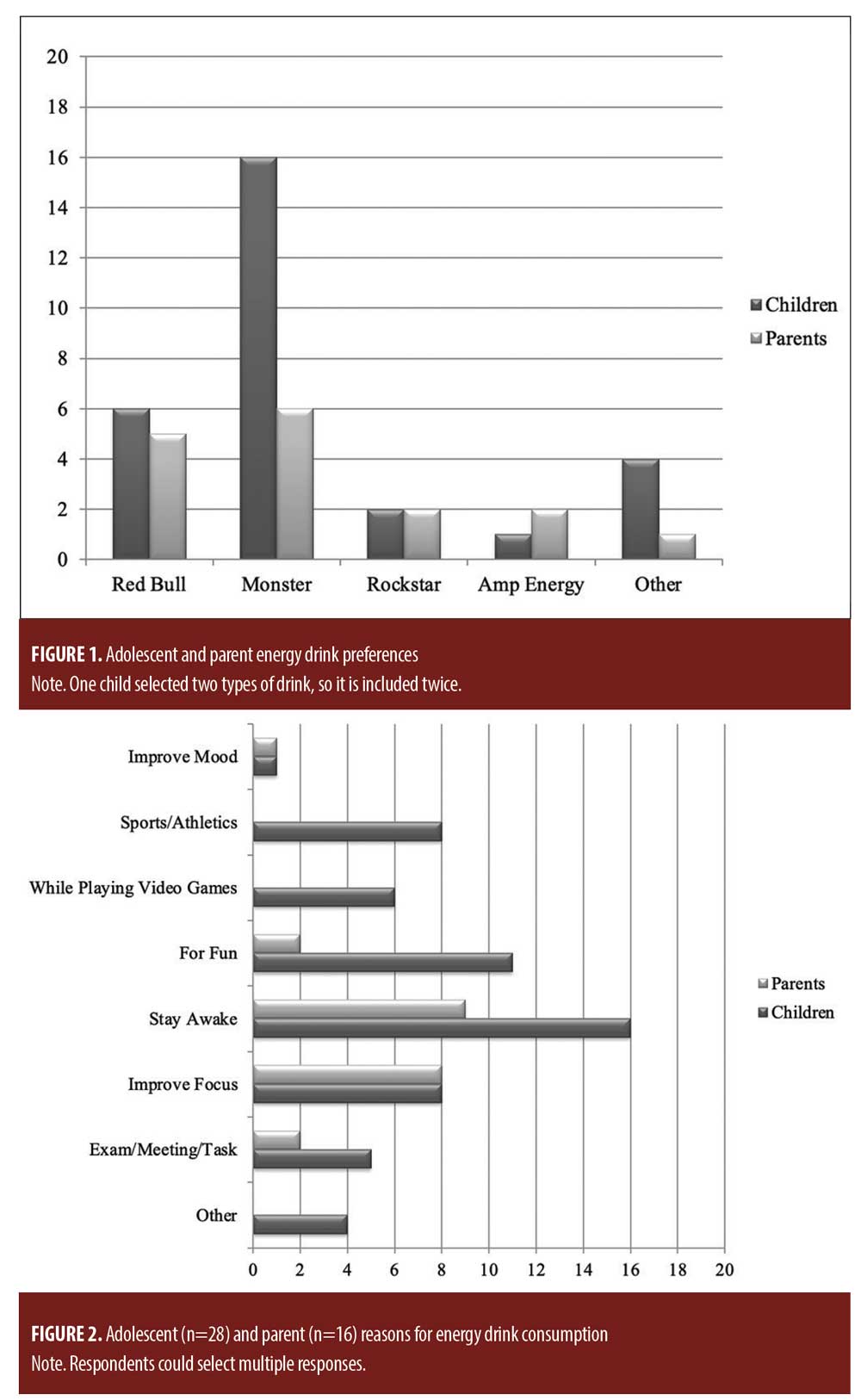
Adolescent and parent preferences for brand of energy drink were similar, with the exception of Monster, which was preferred by more adolescents than adults (Figure 1). Among youth, the most common reasons listed for energy drink consumption were to improve wakefulness (n=16), for fun (n=11), for energy to engage in sports/athletics (n=8), and to improve their focus (n=8). Among parents, the top reason provided for energy drink consumption was to improve wakefulness (n=9), followed by improving focus (n=8), to participate in a meeting, exam, or task, (n=2); and for fun (n=2) (Figure 2).
Discussion
Study findings did not indicate a statistically significant difference in energy drink consumption in adolescents with ADHD compared to age-matched non-ADHD peers. This is contrary to our expectations at the beginning of the study. We anticipated that adolescents diagnosed with ADHD would consume energy drinks at a higher rate than their non-ADHD peers. Adolescents of parents who reported consuming energy drinks had a higher rate of energy drink consumption compared to adolescents of parents who denied consuming energy drinks. This association between consumption rates of parents and their children is of concern, even in this small sample.
From 2003 to 2008, energy drink consumption among adolescents increased by 16 percent, and 35 percent of teenagers reported regular consumption of energy drinks.10 With beverage companies widening their target market for energy drinks and advertising now focusing on youth and women,6 adolescent energy drink consumption rates could soon match adult usage if this trend continues. In this study, most parents (76%) reported being aware of their child’s energy drink usage. Such a high rate suggests that many parents are unaware of the serious risks that have been associated with energy drink consumption in adolescents.
The frequency of energy drink consumption reported in this study was lower than what has been reported in other studies,15 with adolescents reporting that they consumed just one (0.96±1.9 beverages) energy drink in the last week. This finding may be a reflection of the predominantly lower socioeconomic background of respondents, in which the cost of energy drinks may have played a factor. The most expensive sugar sweetened beverages on a per-volume basis are energy drinks, which cost 20.7 cents per ounce, on average, while regular soda ranged from 2.5 to 7.2 cents per ounce.18 A large portion (43%) of adolescents reported that they tried energy drinks for the first time between the ages of 10 and 13 years. This finding is concerning, because nearly half of the participants first tried energy drinks at a young age. Given the caffeine content and other ingredients in energy drinks that may affect health, the potential for adverse events is higher in the younger age groups.19 Both adolescents and parents in this study reported that the main reason for using energy drinks was to stay awake. This could be due to social modeling, with parent behavior directly influencing use of caffeine in their children, or a reflection of the busy culture in Western society, with parents and adolescents expected to accomplish more work and school tasks in a given week. Survey findings were consistent with previous research in that adolescents described their energy drink consumption mostly in the context of social settings.
No therapeutic benefits of energy drinks have been discussed in the literature. Many of the common ingredients in energy drinks are as yet understudied, underreported, and unregulated. The known and unknown pharmacology of ingredients in energy drinks, combined with reports of toxicity and adverse events in high frequency users, raises concern for serious adverse medical or psychiatric effects associated with energy drink use, especially in children and adolescents. Medical professionals and patient advocates should be aware of the possible health implications of energy drink consumption among adolescents and should aid in the education of parents. Our study showed that most parents are aware of and therefore tacitly approve of their adolescent child’s energy drink consumption. Future research should focus on understanding the effects of energy drink use in adolescent populations. Regulation of energy drink sales, marketing, and consumption should be informed by evidence-based research. The FDA recently indicated that it would reexamine the safety of caffeine in the food supply;20 however, more research is needed to better understand patterns of consumption of energy drinks and caffeine among adolescents, as well as the long-term effects of caffeine and energy drink ingredients on overall medical and psychological health.
Limitations. Not all items on the adolescent and parent versions of the current study were well validated, which may influence the findings. Parents who did not respond to the item asking if they were a parent or guardian (n=37) were assumed to be a parent or guardian and were included in analyses. This assumption may not have been correct and could have influenced the findings about parent knowledge of adolescent energy drink consumption. There was missing data that may have skewed some of the findings. It was not possible to compare adolescent reports of mean number of drinks per week to parent reports of their children’s consumption due to incomplete parent surveys. Complete data from surveys would have provided potentially greater confirmation of parent knowledge of their children’s energy drink usage. A final factor in improving survey completion includes more involved training of clinic staff in how to distribute and explain the survey, the study, and instructions for completing the survey accurately. Administrators could also have scanned the forms to be sure that surveys were completed in their entirety.
Conclusion
This survey found that adolescents whose parents consume energy drinks were more likely to drink energy drinks themselves. It appeared that adolescents whose parents denied use of energy drinks were less likely to consume energy drinks. As a nation, 12 percent of adolescents report daily consumption of energy drinks,16 while the prevalence of consuming other sugar-sweetened beverages, such as soft drinks (51%) and fruit drinks (23%), remains much higher in this age group.2, 16 Trends indicate that consumption of energy drinks is increasing in the adolescent population, with potential for serious adverse events resulting from high caffeine content, warranting a need for a public health concern. Medical professionals, nutritionists, teachers, parents, and patient advocates can impact public health policies through continued advocacy addressing the marketing and availability of energy drinks for youth. These professionals can assist in educating parents and youth about the potential complications associated with intake of energy drinks and encourage healthier beverage choices. It would be of public health concern to continue gathering data and conduct further research on energy drink consumption in the adolescent population in order to guide public health policies in the future.
References
- Bedi N, Dewan P, Gupta P. Energy drinks: potions of illusion. Indian Pediatr. 2014 Jul 8;51(7):529–533.
- Seifert SM, Schaechter JL, Hershorin ER, Lipshultz SE. Health effects of energy drinks on children, adolescents, and young adults. Pediatrics. 2011;127(3):511–528.
- Reissig CJ, Strain EC, Griffiths RR. Caffeinated energy drinks: a growing problem. Drug Alcohol Depend. 2009;99:1–10.
- Datamonitor (2004). Global Functional Drinks. Datamonitor Plc. http://www.datamonitor.com/. Accessed Dec 2016
- Lal, GG. Getting specific with functional foods. Food Technology. 2007;61(12):25–31.
- Blankson KL(1), Thompson AM, Ahrendt DM, Patrick V. Energy drinks: what teenagers (and their doctors) should know. Pediatr Rev. 2013 Feb;34(2):55–62.
- Heckman MA, et al. Caffeine (1, 3, 7-trimethylxanthine) in foods: a comprehensive review on consumption, functionality, safety, and regulatory matters. Journal of Food Science. 2010;75:R77.
- Yunusa I, Ahmed IM. Energy drinks: composition and health benefits. Bayero J Pure Applied Sci. 2011;4:186–191.
- Oddy WH, O’Sullivan TA. Energy drinks for children and adolescents, erring on the side of caution may reduce long term health risks. BMJ. 2009;339:b5268.
- Malinauskas BM, Aeby VG, Overton RF, Carpenter-Aeby T, Barber-Heidal K. A survey of energy drink consumption patterns among college students. Nutr J. 2007;6(6):35.
- Costa BM, Hayley A, Miller P. Young adolescents’ perceptions, patterns, and contexts of energy drink use. A focus group study. Appetite. 2014 Sep;80:183–189.
- Schaumburg H, Kaplan J, Windebank A, et al. Sensory neuropathy from pyridoxine abuse. A new megavitamin syndrome. N Engl J Med. 1983; 309:445–448.
- Starling S. Energy Drinks Safety Questioned by German Agency. Beverage Daily. beveragedaily.com. Published 2008.
- Berger AJ, Alford K. Cardiac arrest in a young man following excess consumption of caffeinated ‘energy drinks’. Med J Aust. 2009;190:41–43.
- Bunting H, Baggett A, Grigor J. Adolescent and young adult perceptions of caffeinated energy drinks. A qualitative approach. Appetite. 2013;65:132–138.
- Han E, Powell L. Consumption patterns of sugar-sweetened beverages in the United States. J Acad Nutr Diet. 2013;113:43–53.
- Yunusa I, Ahmed IM. Energy drinks: composition and health benefits. Bayero J Pure Applied Sci. 2011;4:186–191.
- Powell LM, Isgor Z, Rimkus L, Chaloupka FJ. Sugar-sweetened beverage prices: estimates from a national sample of food outlets. Chicago, IL: Bridging the Gap Program, Health Policy Center, Institute for Health Research and Policy, University of Illinois at Chicago, 2014. www.bridgingthegapresearch.org.
- Seifert SM(1), Seifert SA, Schaechter JL, Bronstein AC, Benson BE, Hershorin ER, Arheart KL, Franco VI, Lipshultz SE. An analysis of energy-drink toxicity in the National Poison Data System. Clin Toxicol (Phila). 2013 Aug;51(7):566–574.
- Caffeine and kids: FDA takes a closer look. https://www.fda.gov/consumers/consumer-updates/caffeine-and-kids-fda-takes-closer-look. Updated 3 May 2013. Accessed 11 July 2020.