
 by Atmaram Yarlagadda, MD; Megan A. Connell, PsyD; Jayaprada Kasaraneni, MBBS; and Anita H. Clayton, MD
by Atmaram Yarlagadda, MD; Megan A. Connell, PsyD; Jayaprada Kasaraneni, MBBS; and Anita H. Clayton, MD
Dr. Yarlagadda is Chief, Behavioral Health Services, McDonald Army Health Center in Newport News, Virginia, and Assistant Professor, Department of Psychiatry and Neurobehavioral Sciences, University of Virginia, Charlottesville, Virginia; Dr. Connell is Officer in Charge, Behavioral Health Services, McDonald Army Health Center in Newport News, Virginia; Dr. Kasaraneni is Research Assistant, Vaccine and Gene Therapy, Oregon Health and Science University, Portland, Oregon; and Dr. Clayton is Professor, Department of Psychiatry, University of Virginia, Charlottesville, Virginia.
Innov Clin Neurosci. 2013;10(11–12):19–22
Funding: No funding was received for the preparation of this article.
Financial disclosures: The authors have no conflicts of interest relevant to the content of this article. The views expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Department of Defense, US Army or the Government
Key words: insomnia, ADHD, obesity, breathing problems, pediatrics.
Abstract: Attention deficit hyperactivity disorder is a commonly diagnosed condition in the pediatric as well as adult psychiatric population. Attention deficit hyperactivity disorder has undoubtedly been over diagnosed and treated with both stimulants and non-stimulants over the past few decades. Behavior problems in children are commonly noticed both by parents and teachers, leading to the formulation of attention deficit hyperactivity disorder diagnosis. Insomnia, on the other hand, is not as readily detected by parents and may result in behavioral problems at school. Several medical conditions responsible for causing insomnia may need to be ruled out before the diagnosis of attention deficit hyperactivity disorder is confirmed. In this article, we highlight symptoms common both to insomnia and attention deficit hyperactivity disorder by development of a checklist to help delineate the two conditions. The purpose of this checklist is to provide informational and educational tools both for parents and teachers to distinguish insomnia from attention deficit hyperactivity disorder. The ultimate goal of this paper is to improve diagnostic screening for attention deficit hyperactivity disorder by excluding conditions such as insomnia that may masquerade as attention deficit hyperactivity disorder.
Background
The association of attention deficit hyperactivity disorder (ADHD) with insomnia is well cited in literature;[1–3] however, the significance of this association is not well documented in the exclusionary diagnostic criteria listed in the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM) for either condition.[4] Clinically, the most common condition mimicking ADHD symptoms results from complications related to insomnia/sleep disturbances, whether primary or secondary in origin.[5] Inability to recognize insomnia may lead to confusion of clinical symptoms of irritability, hyperactivity, forgetfulness, and lack of attention, focus and concentration, with ADHD.[6] While most adults have the ability to verbalize symptoms of insomnia, children are unlikely to complain, but rather act out, presenting with behavioral problems resulting from fatigue and sleep deprivation.[7] Therefore, insomnia in children is a clinically important diagnostic consideration before confirming the diagnosis of ADHD, as insomnia can be reversible.
Common reversible causes of insomnia in children include breathing-related sleep disorders and nonbreathing related factors.[8] Examples of breathing-related sleeping disorders are A) obstructive sleep apnea (OSA), B) nasal septal deviation (NSD) and nasal fractures,[9] C) adenoid hyperplasia/enlarged tonsils, and D) asthma and bronchitis. Nonbreathing-related factors may include A) chronic pain, B) psychiatric conditions, C) exposure to unhealthy foods, D) substance abuse, E) medications, and F) environmental toxins.
Diagnosis
Symptoms of insomnia often mimic symptoms of ADHD in children; however, the two conditions can be differentiated by educating parents with the help of a proposed screening tool. Below is the list of secondary conditions causing insomnia that may result in ADHD like symptoms.
OSA. OSA is now common among children with obesity, and correlation of ADHD in children with obesity and OSA is gaining recognition.[10] Symptoms of OSA, such as snoring, choking, and fatigue, are noticeable, but frequently ignored by parents. Insomnia-related complications experienced by children during the day/at school, such as fatigue, lack of attention, focus, and concentration, are perceived and frequently reported as symptoms of ADHD by teachers.[11]
Nasal septal defects and nasal fractures. Nasal septal defects and nasal fractures are examples of anatomical defects of the septum that can cause chronic trouble breathing, which in turn may lead to insomnia and thus may present as symptoms of ADHD in primary care settings.[12] However, a careful examination of patient history could help clarify and rule out the diagnosis.
Adenoid hyperplasia and enlarged tonsils. Adenoid hyperplasia and enlarged tonsils are very common among children and are known to obstruct the airway causing congestion and difficulty breathing, potentially keeping children awake at night.[13,14]
Bronchial asthma and bronchitis. Bronchial asthma and bronchitis are major causes of insomnia in children, especially in combination with allergies and treatments associated with sleep/wake cycle disturbances.
Pain. Pain, either acute or chronic due to infections, illnesses, or injuries, is another potential contributor to increased discomfort and irritability leading to sleep disturbances.[15,16]
Psychiatric disorders. Psychiatric disorders, such as nocturnal enuresis/encopresis, parasomnias, tics, seizures, anxiety, depression, eating disorders, bipolar disorders, and schizophrenia, are serious concerns that, in pediatrics, could lead to secondary causes of insomnia. Psychiatric illness needs to be ruled out in children with insomnia, as ADHD is a comorbidity associated frequently with other psychiatric conditions.[17–20]
Poor diet. Poor diet includes unhealthy eating such as high sugar and caffeine-containing drinks near bedtime, resulting in stimulation and hyperactivity, thus decreasing restful sleep.[21] Poor sleep hygiene (e.g., use of computers before bed, sleeping with lights or electronics on, inconsistent sleep hours) may also result in symptoms resembling ADHD.
Substance abuse/exposure to toxic substances. Substance abuse[22] and exposure to toxic substances[23] in children have significant impact on a child’s behavior and are well described in literature. Alcohol abuse is frequently comorbid with ADHD and is a major concern in adolescents.[24] Insomnia due to substance abuse may further increase ADHD-like symptoms.
Exposure to cigarette smoke, environmental pollutants, and alcohol (i.e., fetal alcohol syndrome)[25] are other potential causes for concern for insomnia.
Medications. Medications, both prescription and over the counter, can play a major role in sleep regulation in children as well as adults.[26] Monitoring of dosings, timings, and concerns for abuse are critical in sorting associated behavioral changes.
Checklist
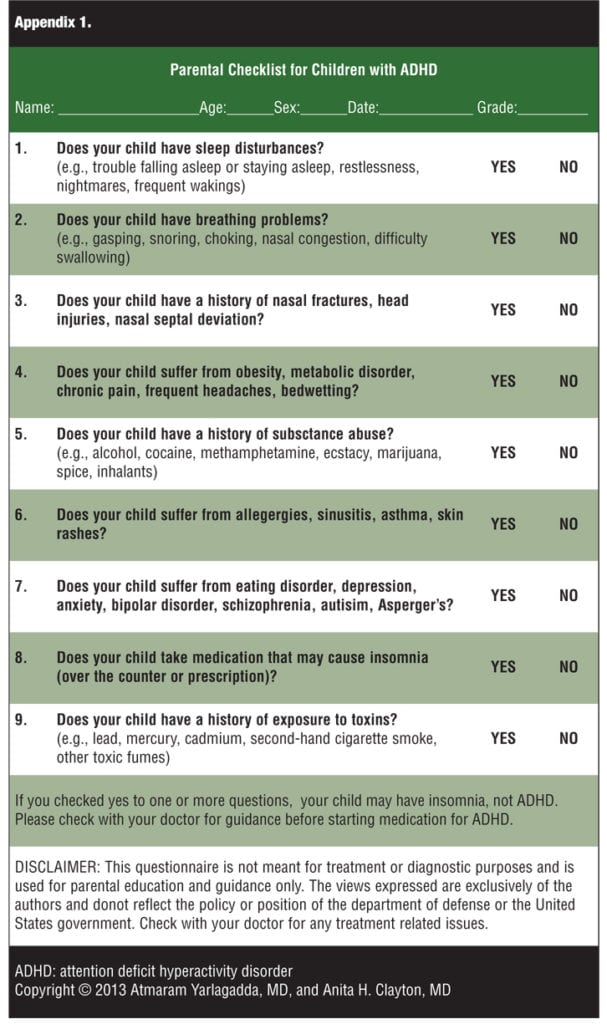
The aim of the proposed checklist is to improve the ability to diagnose and differentiate patients suffering from insomnia presenting as ADHD. Determination of underlying condition by ruling out potential differential diagnoses raises the accuracy of the target diagnosis, in this case ADHD. Exclusionary criteria, therefore, can play essential role in identification of both conditions. The checklist (Appendix 1) consists of nine simple questions with ‘yes or no’ responses to identify the conditions that commonly present with similar symptoms.
Conclusion
We hypothesize that, dimensional outlook as opposed to current categorical approach, may have more relevance in the accurate diagnosis of psychiatric disorders such as ADHD and insomnia. Meanwhile, we hope that introduction of the proposed checklist to the general public and clinicians alike may contribute to reduction in the rapid increase of diagnosis and unwarranted treatment of ADHD both in children as well as adults.
References
1. Faraone SV, Antshel KM. Diagnosing and treating attention-deficit/hyperactivity disorder in adults. World Psychiatry. 2008; 7(3):131–136.
2. Biederman J. Attention deficit hyperactivity disorder: a selective overview. Biol Psychiatry. 2005.;57(11):1215–1220.
3. Calhoun SL, Fernandez-Mendoza J, Vgontzas AN, et al. Prevalence of insomnia symptoms in a general population sample of young children and preadolescents: gender effects. Sleep Med. 2014 Jan;15(1):91–95.
4. Cassoff J, Wiebe ST, Gruber R. Sleep patterns and the risk for ADHD: a review. Nat Sci Sleep. 2012;4: 73–80.
5. Arman AR, Ersu R, Save D, et al. Symptoms of inattention and hyperactivity in children with habitual snoring: evidence from a community-based study in Istanbul. Child: Care, Health and Development. 2005;31(6):707–17.
6. American Psychiatric Association Diagnostic and Statistical Manual of Mental Disorders. 4th ed. Text Revision. Washington, DC: American Psychiatric Association; 2000.
7. Weiss MD, Salpekar J. Sleep problems in a child with ADHD. CNS Drugs. 2010;24(10):811–828.
8. Katz ES, Marcus CL. Diagnosis of obstructive sleep apnea syndrome in infants and children. In: Sheldon SS, Ferber R, Kryger MH (eds). Principles and Practice of Pediatric Sleep Medicine. Philadelphia, PA: Sanders;2005:197–210.
9. P. Rombaux – G. Liistro – M. Hamoir – B. Bertrand – G. Aubert – T. Verse – D. Rodenstein. Nasal obstruction and its impact on sleep-related breathing disorders. Rhinology International Journal. 2005Dec;43(4):242–50.
10. Youssef NA, Ege M, Angly SS, Strauss JL, Marx CE. Is obstructive sleep apnea associated with ADHD? Annals of Clinical Psychiatry. 2011Aug;23(3):213–24.
11. Blesch L, Breese McCoy SJ. Obstructive Sleep Apnea Mimics Attention Deficit Disorder. Journal of Attention Disorders. 2013Mar 25.[Epub ahead of print].
12. Erler T, Paditz E. Obstructive sleep apnea syndrome in children: a state-of-the-art review. Treatments in respiratory medicine. 2004;3(2):107–22.
13. Greenfeld M, Tauman R, DeRowe A, Sivan Y. Obstructive sleep apnea syndrome due to adenotonsillar hypertrophy in infants. International Journal of Pediatric Otorhinolaryngology. 2003Oct;67(10):1055–60.
14. Verhulst SL, Van Gaal L, De Backer W, Desager K. The prevalence, anatomical correlates and treatment of sleep-disordered breathing in obese children and adolescents. Sleep medicine reviews. 2008Oct;12(5):339–46. Epub: 2008 Apr 2011.
15. Salazar A, Dueñas M, Mico JA, Ojeda B, Agüera-Ortiz L, Cervilla JA, Failde I. Undiagnosed Mood Disorders and Sleep Disturbances in Primary Care Patients with Chronic Musculoskeletal Pain. Pain Medicine. 2013Jun6.
16. Kawada T. Regarding “Is shoulder pain for three months or longer correlated with depression, anxiety, and sleep disturbance?” Journal of Shoulder and Elbow Surgery. 2013May7.
17. Smith MT, Haythornthwaite JA. How do sleep disturbance and chronic pain inter-relate? Insights from the longitudinal and cognitive-behavioral clinical trials literature. Sleep Medicine Reviews. 2004Apr;8(2):119–32.
18. Suzuki M, Konno C, Furihata R, Osaki K, Uchiyama M. Insomnia associated with psychiatric disorders. Japanese Journal of Clinical Medicine. 2009Aug; 67(8):1507–12.
19. Riemann D. Insomnia and comorbid psychiatric disorders. Sleep Medicine. 2007 Dec;8 Suppl 4:S15–20.
20. Kai Spiegelhalder,Wolfram Regen, Svetoslava Nanovska, Chiara Baglioni, Dieter Riemann. Comorbid Sleep Disorders in Neuropsychiatric Disorders Across the Life Cycle. Current Psychiatry Reports. May 2013, 15:364
21. Tanaka E, Yatsuya H, Uemura M, Murata C, Otsuka R, Toyoshima H, Tamakoshi K, Sasaki S, Kawaguchi L, Aoyama A. Associations of protein, fat, and carbohydrate intakes with insomnia symptoms among middle-aged Japanese workers. Journal of Epidemiology. 2013; 23(2): 132–8. Epub 2013 Feb 16.
22. Elkins IJ, McGue M, Iacono WG. Prospective effects of attention-deficit/hyperactivity disorder, conduct disorder, and sex on adolescent substance use and abuse. Archives of General Psychiatry. 2007 Oct; 64(10): 1145–52.
23. Curtis LT, Patel K. Nutritional and environmental approaches to preventing and treating autism and attention deficit hyperactivity disorder (ADHD): a review. Journal of alternative and complementary medicine. 2008 Jan-Feb;14(1):79–85.
24. an Emmerik-van Oortmerssen K, van de Glind G, van den Brink W, Smit F, Crunelle CL, Swets M, Schoevers RA. Prevalence of attention-deficit hyperactivity disorder in substance use disorder patients: a meta-analysis and meta-regression analysis. Drug and Alcohol Dependence. 2012 Apr 1; 122(1-2):11–9.
25. Chen ML, Olson HC, Picciano JF, Starr JR, Owens J. Sleep problems in children with fetal alcohol spectrum disorders. Journal of Clinical Sleep Medicine. 2012 Aug15;8(4):421–9.
26. Holvoet E, Gabriëls L. Disturbed sleep in children with ADHD: is there a place for melatonin as a treatment option? Tijdschr Psychiatr. 2013;55(5):349–57.