
Innov Clin Neurosci. 2026;23(4–6):40–43.
By Micaela Dines, MD; Paloma Bamondez, MD; Micaela Montenegro, MD; Pablo Diaz, MD; Ana Laura Ramos, LP; Irene Luis Vega; Gustavo Vazquez, MD, PhD; and Adriana Bulacia, MD
Drs. Dines, Bulacia, Bamondez,, and Diaz are with the Mental Health Section, Department of Medicine, Hospital General de Agudos Dr. Juan A. Fernandez, Buenos Aires, Argentina. Dr. Dines is additionally with the Institute of Cognitive and Translational Neuroscience, National Council of Scientific and Technical Research – INECO Foundation – Favaloro University, Buenos Aires, Argentina. Dr. Bamondez is additionally with the Institute of Cognitive Neuroscience-INECO, Buenos Aires, Argentina. Dr. Luis Vega is additionally with the Division of Anesthesia, Analgesia and Resuscitation, Department of Medicine, Hospital General de Agudos Dr. Juan A. Fernández, Buenos Aires, Argentina. Dr. Montenegro and Psychologist Ana Laura Ramos are with the Division of Toxicology, Department of Emergency Medicine, Hospital General de Agudos Dr. Juan A. Fernández, Buenos Aires, Argentina. Dr. Vazquez is with the Department of Psychiatry, School of Medicine at Queen’s University, Kingston, Ontario, Canada; and the International Consortium for Mood & Psychotic Disorder Research, McLean Hospital, Belmont, Massachusset.
FUNDING: No funding was provided for this article.
DISCLOSURES: The authors have no relevant conflicts of interest.
Abstract: Treatment-resistant depression (TRD) is a severe form of depression associated with high rates of disability and suicide, underscoring the need for effective therapeutic alternatives. In recent years, subanesthetic intravenous (IV) ketamine has emerged as a promising intervention due to its rapid antidepressant and antisuicidal effects. This report describes the case of a 41-year-old male patient with TRD treated with IV ketamine at a public hospital in Argentina—the first such reported case in this setting. We detail the diagnostic process, treatment protocol, outcomes, and practical considerations in implementing this novel therapy within a public health system. Keywords: Depression, ketamine, treatment-resistant depression, neuromodulation
Introduction
Treatment-resistant depression (TRD) represents a significant clinical challenge; patients with TRD do not achieve adequate remission despite the use of conventional therapeutic strategies, which leads to an intense search by the treating professional for other strategies to achieve symptomatic remission. Approximately 30% of patients diagnosed with major depressive disorder (MDD) will experience TRD and consequently will be exposed to an increased risk of functional impairment, psychiatric and physical comorbidities, and increased suicidal ideation and behavior.1 Therefore, as psychiatrists, we need to know what other strategies are available to achieve symptomatic remission in patients with TRD.
The search for more effective therapeutic alternatives has led to the development of innovative approaches, among which intravenous (IV) ketamine has emerged as a promising option, mainly because of its clinical effects within hours or days.2 The introduction of IV ketamine as a treatment in psychiatry constitutes a significant milestone and a true paradigm shift in the approach to TRD. Traditionally, psychiatry has focused on oral pharmacological treatments and psychological therapies. However, IV ketamine has broken new ground, offering a rapid and effective response for those patients who do not find relief from conventional treatments.
This breakthrough represents much more than adding a new drug to the therapeutic arsenal; it signifies a profound transformation in our understanding of depression and how we can treat it. Ketamine at subanesthetic doses acts differently from traditional antidepressants by modulating the glutamatergic system and promoting neuroplasticity.3 This novel mechanism of action allows us to obtain rapid and sustained results. This treatment offers a paradigm shift that invites us to explore new frontiers in psychiatry and renew hope for patients struggling with depression, opening the door to a better quality of life and emotional wellbeing.
In this article, we present a case report of the use of IV ketamine in the treatment of TRD in January 2025 at the Hospital General de Agudos Dr. Juan A. Fernández in Buenos Aires, Argentina. To our knowledge, this was the first such case reported in a public hospital in our country.
Clinical case
Clinical history. A 41-year-old male patient was referred to the Ketamine for Depression Clinic of the Hospital General de Agudos Dr. Juan A. Fernández by his treating psychiatrist, presenting with a diagnosis of TRD. Once admitted, the diagnosis of TRD was re-evaluated through joint interviews with family members. The interviews were accompanied by the application of clinical scales, including the Montgomery–Åsberg Depression Scale4 (MADRS) and Beck Depression Inventory5 (BDI-II), and screening scales for bipolar disorder, including the Bipolar Spectrum Diagnostic Scale (BSDS) and Mood Disorder Questionnaire (MDQ). The pertinent complementary studies were performed to rule out pseudoresistance. The patient had presented a depressive episode at the age of 35 years with complete remission of symptoms after conventional treatment with antidepressants. He had 2 suicide attempts with amnesia of the episode in the context of a confusional disorder following alcohol and clonazepam consumption and a voluntary hospitalization in August 2024 for affective lability and lack of response to the treatment. He did not present affective episodes before the age of 25 years and did not have a family history of affective disorders or other relevant antecedents.
At the time of admission to treatment, the patient had complementary studies, including complete laboratory tests, electroencephalogram, electrocardiogram (ECG), and magnetic resonance imaging of the brain with no particularities. Likewise, a neuropsychological evaluation was performed, including the Signoret Mnemic Efficacy Battery, the Stroop Test, Trail Making Test, and the Symbol Search, Number Key, Digit Key and Arithmetic subtests of the Wechsler Adult Intelligence Scale-4th edition. The selected test battery aims to assess the cognitive functions that are usually affected in this diagnosis6 as well as to establish a cognitive baseline to compare changes and measure the impact of the treatment in terms of detecting improvements or deteriorations in the monitored functions.
Regarding previous treatments, the patient received more than 2 antidepressants at maximal doses and for more than 8 weeks each; these included bupropion, venlafaxine, escitalopram, and desvenlafaxine. The diagnosis of bipolar disorder was ruled out, confirming the diagnosis of TRD proposed by the treating psychiatrist.
Having exhausted the therapeutic alternatives available in our hospital, the use of IV ketamine at subanesthetic doses was proposed to the patient as a combination therapy to his current treatment with desvenlafaxine 100 mg,bupropion XR 450 mg, lithium XR 900 mg, divalproex sodium 100 mg, quetiapine XR 300 mg and 2.5 mg of lorazepam provided by his general psychiatrist. Authorization was requested from the hospital Ethics Committee, the hospital director, and the pharmacy department, and they drafted a protocol for the application, safety, and traceability of ketamine and supervised it.
Once both the patient and his relatives received information on the risks and benefits of the treatment, as well as alternatives to it, and signed an informed consent, the specialized treatment was started.
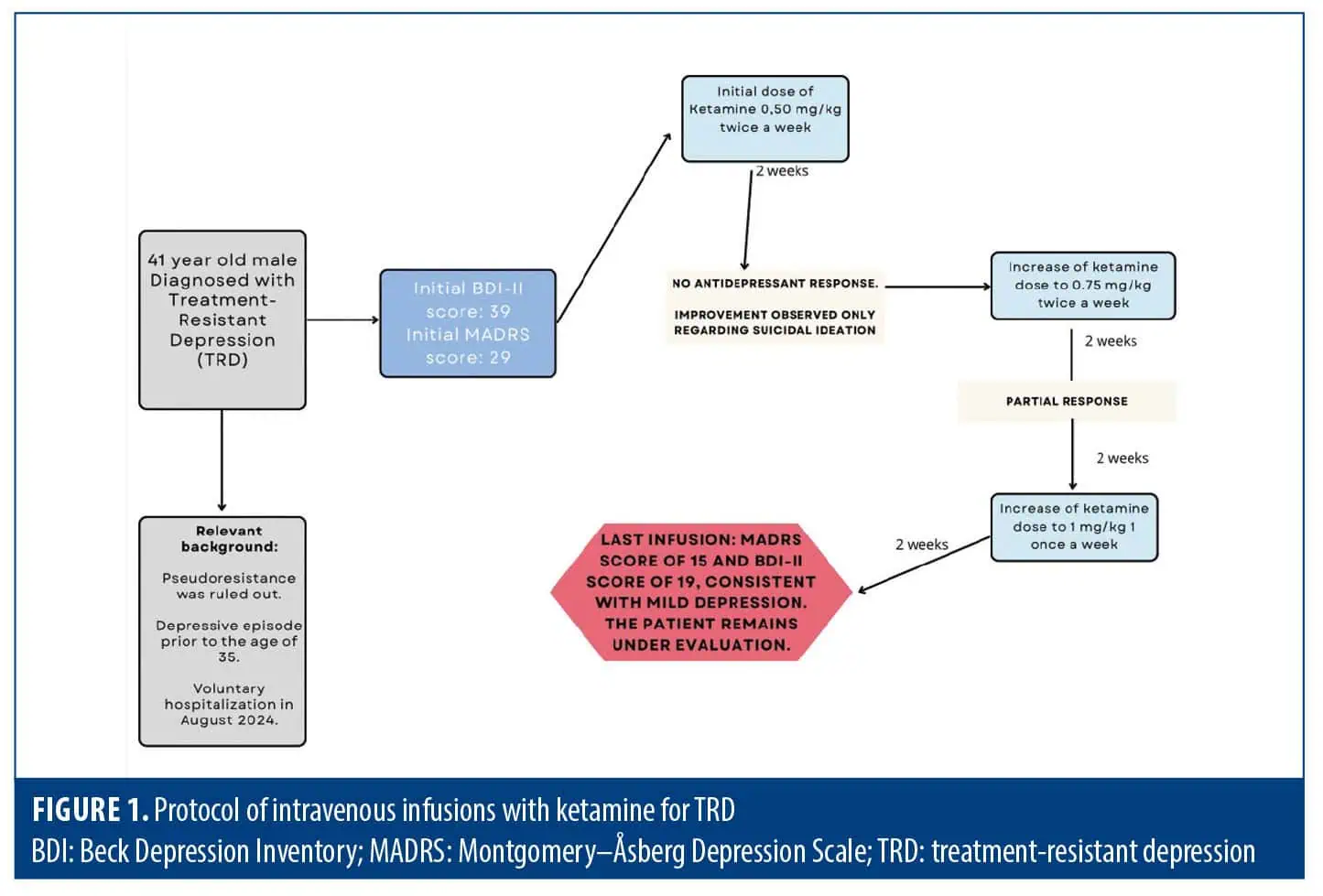
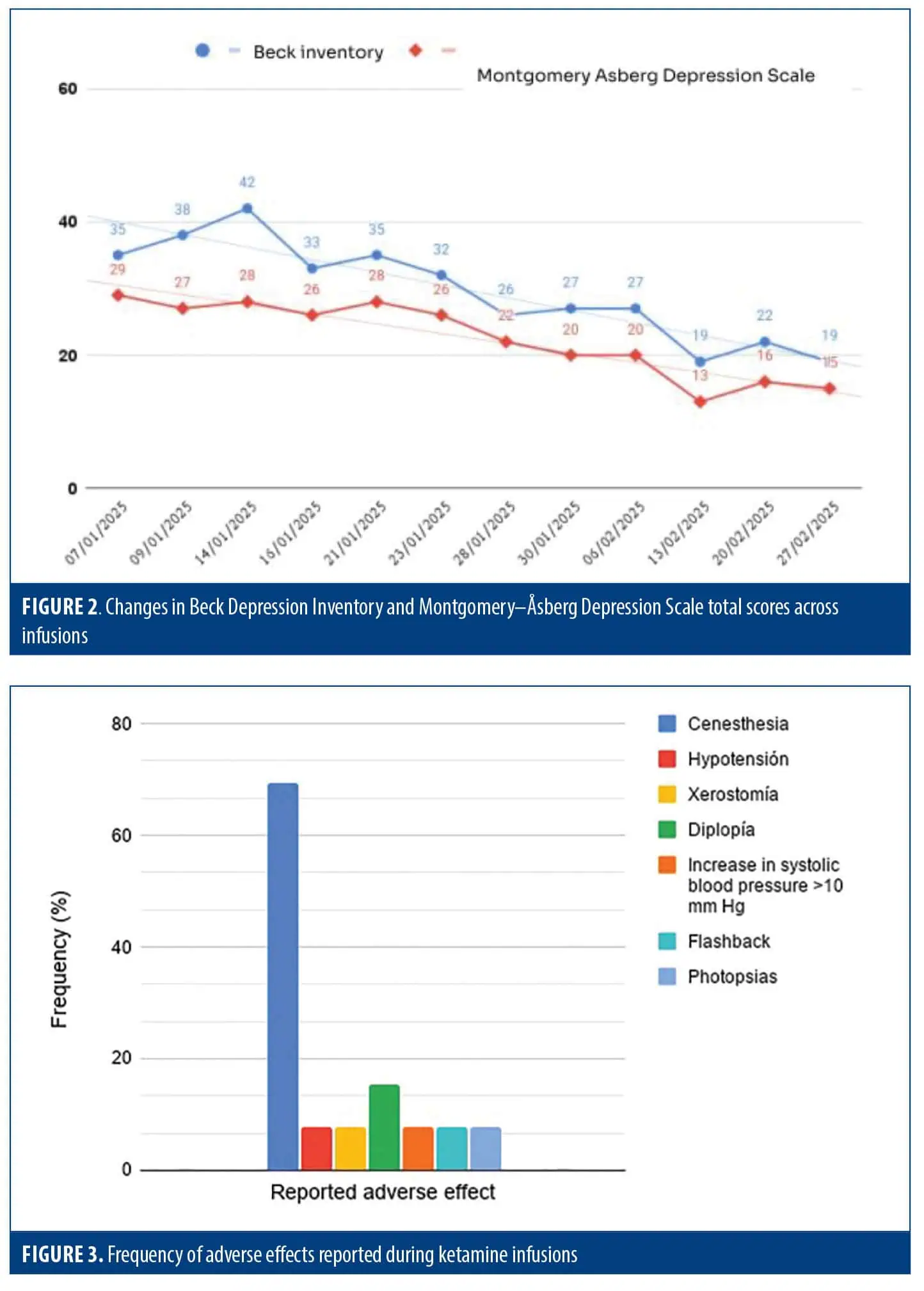
IV ketamine infusions. An infusion protocol was developed7 based on the Canadian Network for Mood and Anxiety Treatments (CANMAT) guidelines8 and international consensus3 as well as the protocol for the application of intravenous infusions for mood disorders of the Mood Disorder Service of Providence Care Hospital in Kingston, Ontario, Canada9 and was externally supervised by Dr. Gustavo Vazquez10, an expert in the subject. The patient underwent 8 ketamine infusions (4 infusions at doses of 0.5 mg/kg, 4 at doses of 0.75 mg/kg, and the last 4 infusions at 1 mg/kg) over 12 weeks (Figure 1). Infusions lasted for 40 minutes. The doses were increased according to the patient’s response, which was initially partial on the BDI and MADRS (Figure 2). The patient was asked to discontinue benzodiazepines the night before treatment initiation since they could attenuate the effect of ketamine. No other modifications were made to his usual baseline treatment. Both weight and blood pressure (BP) were measured before each infusion. Monitoring and infusions were performed by trained professionals (anesthesiology, intensive care/emergency room) through a multiparametric monitor. BP, oxygen saturation, ECG, and heart rate were monitored every 15 minutes and reported in the patient’s clinical history. Also present during the infusions were the psychiatrist in charge of the infusion, the ketamine team coordinator, and a nurse in charge of the infusions.
The infusions were performed in a controlled environment with low sensory stimulation to minimize adverse effects such as dissociation or anxiety. The patient wore headphones with music of his choice during the procedure.
BP, oxygen saturation, heart rate, and ECG remained stable throughout the infusions, despite the dose increases. The patient had no serious adverse effects (Figure 3), with the most frequent being the presence of cenesthesia (76.9%), followed by diplopia (15.4%). The patient reported that the experience was pleasant, favoring treatment adherence.
At the end of each infusion, the patient remained in the hospital accompanied by a family member for 1 hour and was administered the 6-item Clinician-Administered Dissociative States Scale11 and an adverse effects questionnaire.
Therapeutic response was monitored through changes in the total scores of MADRS and BDI and consecutive clinical interviews. An initial and rapid clinical improvement was recorded with the 0.50 mg/kg dose at the level of suicidal ideation (configured by ideas of disappearing/wanting to die) of the patient in the second week of treatment. However, it was decided to increase the dose to 0.75 mg/kg during the subsequent 4 infusions, registering a partial response (reduction >25% but <50% of the baseline total scores) at the end of the fourth week of treatment. For this same reason, the dose of ketamine was increased to 1 mg/kg infused once per week for another 4 weeks. At the end of the treatment (total 12 infusions over 8 weeks), the patient presented an improvement in the severity of the scales from major depression (MADRS and BDI totals of 29 and 35 points, respectively) to mild depression (MADRS and BDI totals of 15 and 19 points, respectively), and clear clinical improvement was observed in the psychiatric interview. As part of the post-treatment follow-up, the patient was evaluated 15 days after the end of the infusions, in which no adverse effects from the treatment were reported, but a partial symptomatic recurrence was evidenced during the psychiatric clinical evaluation and a relative increase of MADRS (28 points) and BDI (25 points) scores.
Discussion and Conclusion
Although the implementation of IV ketamine treatment at subanesthetic doses requires specialized knowledge and a multidisciplinary approach, it represents a new tool for the treatment of patients with symptomatology refractory to conventional therapies in depression. Major depression is one of the leading causes of global disability. For those patients who do not respond to conventional treatments, IV ketamine is an effective and safe therapeutic option.2,12 Considering that the possibility of using electroconvulsive therapy is not available in public hospitals in Argentina, IV ketamine infusions at subanesthetic doses represent an extremely valuable tool. It should be noted that although its application is off-label, it is supported by both national and international scientific associations and is also indicated as a treatment for TRD in guidelines such as CANMAT1 and the Argentine Consensus for Diagnosis and Treatment of Refractory Major Depressive Disorder of 202013 as well as in Treatment Resistant Bipolar Depression (TRBD).12 However, it is essential to mention that this procedure should be implemented in specialized healthcare settings and under strict clinical protocols that guarantee its safety and efficacy, minimizing the risks of adverse effects or substance abuse.
The implementation of innovative treatments in mental health not only promotes an interdisciplinary and interventionist approach in the management of mental disorders but also represents a significant advance in equitable access to care in the public health system. Interventions of this type constitute a transcendental step toward health equity by ensuring patients can access effective and safe treatments without facing economic barriers.10 Although this initiative is an encouraging first step for the public health system in our country, it is essential to continue reflecting on how to ensure sustained access to this therapy, evaluate maintenance protocols, promote research in this field, and encourage other hospitals in the public system to incorporate this therapeutic alternative.
Ethics statement
Data were collected and analyzed in compliance with relevant data protection regulations. No personally identifiable information is disclosed in this paper, and the patient has provided written informed consent for publication.
Acknowledgments
We sincerely thank Electromedik S.A. for the donation of the multiparameter monitor, which made this project possible. Mónica Pereyra, Cynthia Cichello, and Laura Natalia Ríos Merino were collaborators on this manuscript.
References
- Lam RW, Kennedy SH, Adams C, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2023 update on clinical guidelines for management of major depressive disorder in adults: Réseau Canadien pour les Traitements de L’humeur et de L’anxiété (CANMAT) 2023: mise à jour des lignes directrices cliniques pour la prise en charge du trouble dépressif majeur chez les adultes. Can J Psychiatry. 2024:7067437241245384.
- McIntyre RS, Alsuwaidan M, Baune BT, et al. Treatment-resistant depression: definition, prevalence, detection, management, and investigational interventions. World Psychiatry. 2023;22(3):394–412.
- McIntyre RS, Rosenblat JD, Nemeroff CB, et al. Synthesizing the evidence for ketamine and esketamine in treatment-resistant depression: an international expert opinion on the available evidence and implementation. Am J Psychiatry. 2021;178(5):383–399.
- Montgomery A, Åsberg M. Scale designed to be sensitive to change. Br J Psychiatry. 1979;134:382–389.
- Beck AT, Kovacs M, Weissman A. Assessment of suicidal intention: the Scale for Suicide Ideation. J Consult Clin Psychol. 1979;47(2):343–352.
- Kriesche D, Woll CFJ, Tschentscher N, Engel RR, Karch S. Neurocognitive deficits in depression: a systematic review of cognitive impairment in the acute and remitted state. Eur Arch Psychiatry Clin Neurosci. 2023; 273(5):
1105–1128. - Dines M, Bulacia A, Bamondez P, et al. [Subanesthetic dose ketamine infusions for treatment-resistant major depression: an application protocol at a public hospital in Argentina]. Vertex. 2025;36(168):33–38. Spanish.
- Swainson J, McGirr A, Blier P, et al. The Canadian Network for Mood and Anxiety Treatments (CANMAT) Task Force recommendations for the use of racemic ketamine in adults with major depressive disorder: recommendations du groupe de travail du Réseau Canadien pour les Traitements de L’humeur et de L’anxiété (Canmat) concernant l’utilisation de la kétamine racémique chez les adultes souffrant de trouble dépressif majeur. Can J Psychiatry. 2021;66(2):113–125. Erratum in: Can J Psychiatry. 2021;66(12):1102.
- Ketamine. Providence Care. 2021. Accessed 6 May 2026. https://providencecare.ca/services-referrals/ketamine/
- Gutierrez G, Kang MJY, Vazquez G. IV low dose ketamine infusions for treatment resistant depression: results from a five-year study at a free public clinic in an academic hospital. Psychiatry Res. 2024;335:115865.
- Rodrigues NB, Mcintyre RS, Lipsitz O, et al. A simplified 6-Item clinician-administered dissociative symptom scale (CADSS-6) for monitoring dissociative effects of sub-anesthetic ketamine infusions. J Affect Disord. 2021;282:160–164.
- Cetkovich-Bakmas M, Abadi A, Camino S, et al. [Third Argentine consensus statement on management bipolar disorders. Section 3: bipolar disorder in the context of special situations]. Vertex. 2023;34(161):87–110. Spanish.
- Corrales A, Cetkovich-Bakmas M, Corral R, et al. [Argentine consensus on the diagnosis and treatment of treatment-resistant major depressive disorder (MDD)]. Vertex. 2020;31:
1–40. Spanish.