
Innov Clin Neurosci. 2015;12(3–4):11–13.
Funding/financial disclosures: No funding was received for this study or for the preparation of this letter. The authors have no conflicts of interest relevant to the content of this letter.
Dear Editor:
Nonadherence to treatment is a “global challenge for psychiatry.”[1]* Despite varying methodologies and definitions of treatment adherence,[2] empirical endeavors and literature reviews have reported compromised adherence in patients with depression,[3–5] bipolar disorder,[3,5,6] anxiety disorders,[7] schizoaffective disorder,[8] schizophrenia,[5,8–10] substance misuse,[11] and attention deficit hyperactivity disorder.[12,13] However, most studies have examined only one psychiatric disorder and only one form of treatment adherence (typically medication). We speculated about possible relationships between general mental health treatment indicators (not specific psychiatric diagnoses) and lower adherence with general healthcare (i.e., not psychiatric treatment).
Participants were men and women, ages 18 years or older, being seen for non-emergent medical care at an internal medicine outpatient clinic staffed predominantly by residents. We excluded individuals with medical (e.g., debilitating pain), intellectual (e.g., intellectual disability), cognitive (e.g., dementia), or psychiatric symptoms (e.g., psychotic) of a severity to preclude the candidate’s ability to successfully complete a survey (n=5: two with vision impairment, two with cognitive impairment, one with intellectual disability). This exclusion process was informal and undertaken by the recruiter as patients registered for clinical service, as surveys needed to be completed before appointments with providers.
This project was reviewed and exempted by the institutional review boards of the sponsoring hospital and the local university. Completion of the survey was assumed to be implied consent, which was explained to participants on the cover page of the survey.
At the outset, 354 individuals were approached and 300 agreed to participate (84.7%). As for the 54 individuals who did not participate, 17 stated too ill, 19 not enough time, 14 “don’t like surveys,” three “pleased with current care” (?), and one “too angry” to participate. Ultimately, 272 participants completed the items necessary for analyses, resulting in 213 (78.3%) women and 59 (21.7%) men, ranging in age from 18 to 89 years (mean [M]=45.37, standard deviation [SD]=13.92). Most participants were White (85.7%); however, 8.5 percent of participants were African-American, 2.2 percent Native American, 0.4 percent Asian, 1.1 percent Hispanic, and 2.2 percent “Other.” All but 5.9 percent had graduated from high school, and 10.7 percent had earned a bachelor’s degree.
During clinic hours, one of the authors (R.J.B.) approached incoming patients following registration, informally assessed exclusion criteria and, with potential candidates, reviewed the focus of the project (i.e., a study examining health and treatment experiences). Each participant was asked to complete onsite in the lobby a five-page anonymous survey, which took about 10 minutes, and to place completed surveys into sealed envelopes and then into a collection box.
The survey consisted of three sections, the first being a demographic query. With yes/no response options, the second section examined participants’ mental health history through general queries about four types of mental healthcare utilization (i.e., “Have you ever been seen by a psychiatrist?” “Have you ever been hospitalized in a psychiatric hospital?” “Have you ever been in counseling?” “Have you ever been on medication for your nerves?”).
The final section of the survey examined various facets of adherence to general medical healthcare using four measures. The first item (author-developed) queried, “In general, how conscientious are you about following through with medical treatment?” with Likert style response options from 1 (very conscientious) to 5 (not conscientious at all). The second item (author-developed) consisted of five queries, each exploring general adherence with various healthcare behaviors (i.e., regular dental check-ups, arrival to doctors’ appointments on time, completion of lab work, adherence with exercise and diet instructions), with five Likert-style response options from 1 (never) to 5 (always) as well as “not applicable.” The third measure examined adherence with medication,by asking, “How often do you have difficulty remembering to take your medication?” with Likert-style responses from 1 (never/rarely) to 5 (all the time). This item was recoded so that higher scores indicated greater ease remembering to take medication. The fourth questionnaire was the Medical Outcomes Study (MOS) General Adherence Items.[14] This scale explores general medical adherence with “my doctor” over the past four weeks, and consists of five items with six Likert-style response options from 1 (none of the time) to 6 (all of the time). Note that with all four measures of healthcare adherence, higher scores indicate higher levels of adherence.
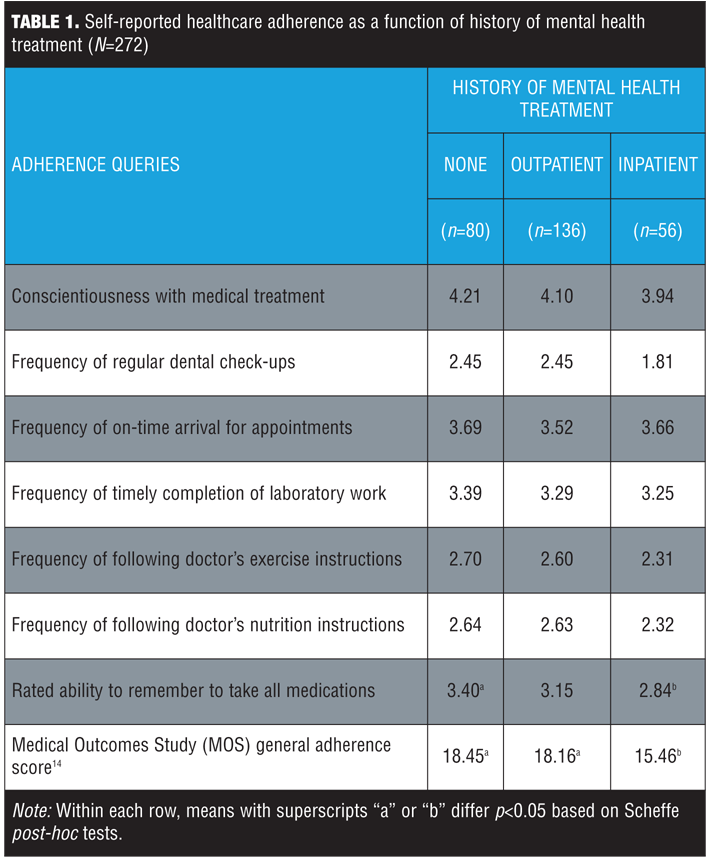
In analyses, 80 (29.4%) participants denied receiving any past mental health treatment, 136 (50%) indicated some form of outpatient treatment (counseling, medications, and/or seen a psychiatrist) but not inpatient treatment, and 56 (20.6%) reported being hospitalized for mental health treatment. Comparisons in healthcare adherence among these three groups are presented in Table 1. Findings indicate few between-group differences with the exception of remembering to take medications and the MOS score, which both demonstrated significant between-group differences between participants with no past mental healthcare and participants with past inpatient treatment. In other words, having a mental health history did not generally predict for adherence issues in the primary care setting, with the exception of past inpatient treatment.
This study has a number of potential limitations, including use of self-report data, the possibility that mental illness may contribute to faulty recollection, small sample size, and recruitment from a resident-provider clinic (possible limitations in generalizing findings to other populations). However, this is the only study to examine multiple adherence variables with medical care in a primary care population, based upon mental health history. Findings suggest that mental health treatment, alone, does not preclude adherence with medical care, with the exception of past inpatient treatment.
References
1. Chapman SC, Horne R. Medication nonadherence and psychiatry. Curr Opin Psychiatry. 2013;26:446–452.
2. Julius RJ, Novitsky MA Jr, Dubin WR. Medication adherence: a review of the literature and implications for clinical practice. J Psychiatr Pract. 2009;15:34–44.
3. Lingam R, Scott J. Treatment non-adherence in affective disorders. Acta Psychiatr Scand. 2002;105:164–172.
4. Sansone RA, Sansone LA. Antidepressant adherence: are patients taking their medications? Innov Clin Neurosci. 2012;9(5–6):41–46.
5. Conti V, Lora A, Cipriani A, et al. Persistence with pharmacological treatment in the specialist mental healthcare of patients with severe mental disorders. Eur J Clin Pharmacol. 2012;68:1647–1655.
6. Moon E, Chang JS, Kim MY, et al. Dropout rate and associated factors in patients with bipolar disorders. J Affect Disord. 2012;141:47–54.
7. Taylor S, Abramowitz JS, McKay D. Non-adherence and non-response in the treatment of anxiety disorders. J Anxiety Disord. 2012;26:583–589.
8. Goff DC, Hill M, Freudenreich O. Strategies for improving treatment adherence in schizophrenia and schizoaffective disorder. J Clin Psychiatry. 2010;71:S20–26.
9. Canas F, Alptekin K, Azorin JM, et al. Improving treatment adherence in your patients with schizophrenia: the STAY initiative. Clin Drug Investig. 2013;33:97–107.
10. Tharani AJ, Farooq S, Saleem F, Naveed A. Adherence to antipsychotic medication: a challenge for client, family and health care providers. J Pak Med Assoc. 2013;63:516–518.
11. Weiss RD. Adherence to pharmacotherapy in patients with alcohol and opioid dependence. Addiction. 2004;99:1382–1392.
12. Caisley H, Muller U. Adherence to medication in adults with attention deficit hyperactivity disorder and pro re nata dosing of psychostimulants: a systematic review. Eur Psychiatry. 2012;27:343–349.
13. Adler LD, Nierenberg AA. Review of medication adherence in children and adults with ADHD. Postgrad Med. 2010;122:184–191.
14. Hayes RD. The Medical Outcomes Study (MOS) Measures of Patient Adherence. http://www.rand.org/content/dam/rand/www/external/health/surveys_tools/mos/mos_adherence_survey.pdf. Accessed on April 14, 2014.
With regards,
Randy A. Sansone, MD; R. Jordan Bohinc, DO; and Michael W. Wiederman, PhD
Dr. Sansone is a Professor in the Departments of Psychiatry and Internal Medicine at Wright State University School of Medicine in Dayton, Ohio, and Director of Psychiatry Education at Kettering Medical Center in Kettering, Ohio. Dr. Bohinc is a resident physician in the Department of Internal Medicine at Kettering Medical Center in Dayton, Ohio. Dr. Wiederman is the Director of Faculty Development at the University of South Carolina School of Medicine-Greenville in Greenville, South Carolina.
*Editor’s note: For additional information on patient nonadherence in psychiatry, see this month’s Risk Management column?“Avoiding Risks with Nonadherent Patients.”