
 by Masaru Nakamura, MD, PhD; Megumi Seki, MD; Yosuke Sato, MD; and Takahiko Nagamine, MD, PhD
by Masaru Nakamura, MD, PhD; Megumi Seki, MD; Yosuke Sato, MD; and Takahiko Nagamine, MD, PhD
Dr. Nakamura is with the Department of Psychiatric Internal Medicine, Dr. Seki is with the Department of Internal Medicine, and Dr. Satoh is with the Department of Psychiatry, Kosekai-Kusatsu Hospital, Hiroshima; and Dr. Nagamine is with the Department of Psychiatric Internal Medicine, Shinseikai-Ishii Memorial Hospital, Iwakuni.
Innov Clin Neurosci. 2016;13(1–2):34–36.
Funding: No funding was received for the preparation of this manuscript.
Financial Disclosures: The authors have no conflicts of interest relevant to the content of this article.
Key Words: Quetiapine, second generation antipsychotic, bradycardia, hypotension
Abstract: Quetiapine is increasingly used for the treatment of behavioral and psychological symptoms of dementia in elderly patients. Among the many potential side effects of second-generation antipsychotics, the sudden onset of cardiac abnormality is a particularly important side effect to consider due its fatal implications. Elderly patients may be particularly vulnerable to these cardiac-related side effects due to the likelihood that they have multiple existing health conditions (e.g., heart disease, high blood pressure, diabetes) as well as age-related changes in their pharmacokinetics and pharmacodynamics and differences in their receptor binding profiles. We present a case of an elderly man with a history of heart disease who developed symptomatic bradycardia and hypotension simultaneously while taking quetiapine. After dose reduction and withdrawal of quetiapine, a time sequential improvement of bradycardia and hypotension monitored by repeated electrocardiogram and blood pressure checks suggests a relationship between the higher dosage of quetiapine and cardiac abnormalities. Other factors such as aging itself and chronic heart failure might be associated with cardiac distress. Elderly patients on quetiapine, particularly at higher dosages, should be continually and closely monitored for any symptoms of cardiac distress.
Introduction
Quetiapine is a second-generation antipsychotic (SGA) that is prescribed for a broad spectrum of psychiatric conditions, including off-label uses for behavioral and psychological symptoms of dementia (BPSD). Among the many potential side effects of SGAs, the sudden onset of cardiac abnormality is a particularly important side effect to consider due its fatal implications. Elderly patients may be particularly vulnerable to these cardiac-related side effects due to the likelihood that they have multiple existing health conditions (e.g., heart disease, high blood pressure, diabetes) as well as age-related changes in their pharmacokinetics and pharmacodynamics and differences in their receptor binding profiles.[1] We present a case of an elderly man with a history of heart disease who developed symptomatic bradycardia and hypotension simultaneously while taking quetiapine.
Case Vignette
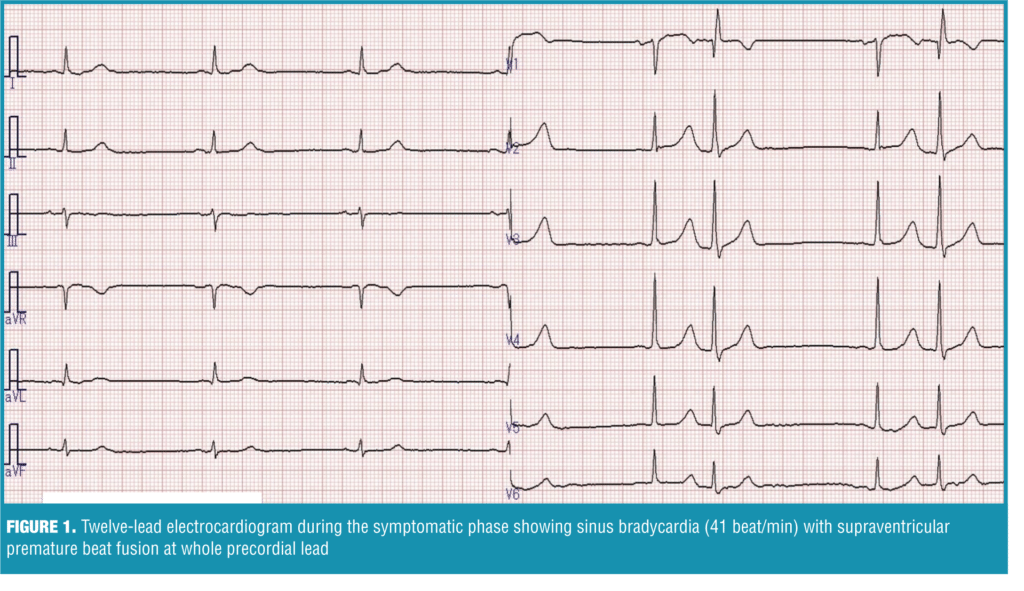
A 72-year-old Japanese male patient with a diagnosis of alcohol dementia was admitted to our hospital’s dementia unit for worsening of BPSD. One month earlier, he had started taking quetiapine (25mg/day) and brotizolam (0.25mg/day) for disorientation and insomnia, and was being treated with furosemide (10mg/day) and spironolactone (25mg/day) for chronic heart failure. At admission, the patient’s pulse rate was 69 beat per minute (bpm), his blood pressure was 122/83mmHg, and a 12-lead electrocardiogram (ECG) showed regular sinus rhythm with minimal QTc interval prolongation (QTc interval=480 msec). His score on Mini-Mental State Examination was 18/30, and there were no particular abnormalities in the physical exam. Laboratory work-up and chest X-ray were all within normal limits except for mild elevation of N-terminal fragment pro-brain type natriuretic peptide (NT-proBNP=302pg/mL). To treat his irritability and aggressiveness, we gradually increased his quetiapine dosage, so that in two weeks, the dosage was 100mg/day. We performed another ECG at this time, which showed a normal sinus rhythm of 60bpm (QTc interval=461 msec). Over the next month, we continued to titrate the quetiapine to the final dosage of 225mg/day, and his psychotic symptoms stabilized. After three months, the patient abruptly complained of sleepiness and feebleness and was noted to have bradysphygmia (48bpm) with low blood pressure (78/44mmHg). An ECG was performed and was suggestive of sinus bradycardia (41bpm , QTc interval=452msec) with supra-ventricular extra-systole rhythm (Figure 1).
 There were no new abnormal findings in the laboratory tests (NT-proBNP=311pg/mL), chest X-ray, and echocardiogram, and the dose escalation of quetiapine was the only medication change he had received since his initial evaluation. Taking into consideration his current and previous ECGs, we suspected that quetiapine at 225mg/day was contributing to his decrease in heart rate and blood pressure. We reduced his quetiapine dosage to 100mg/day. His severe bradycardia and hypotension persisted for about 72 hours without additional internal treatment. Seven days later, a follow-up ECG revealed improvement in bradycardia (50bpm) and blood pressure (110/70mmHg). However, reappearance of irritability and aggressiveness in the patient forced us to fully discontinue the quetiapine and initiate valproic acid at 400mg/day, while his other medications were continued at the same dosages. Over the next month, the severe bradycardia and hypotension resolved.
There were no new abnormal findings in the laboratory tests (NT-proBNP=311pg/mL), chest X-ray, and echocardiogram, and the dose escalation of quetiapine was the only medication change he had received since his initial evaluation. Taking into consideration his current and previous ECGs, we suspected that quetiapine at 225mg/day was contributing to his decrease in heart rate and blood pressure. We reduced his quetiapine dosage to 100mg/day. His severe bradycardia and hypotension persisted for about 72 hours without additional internal treatment. Seven days later, a follow-up ECG revealed improvement in bradycardia (50bpm) and blood pressure (110/70mmHg). However, reappearance of irritability and aggressiveness in the patient forced us to fully discontinue the quetiapine and initiate valproic acid at 400mg/day, while his other medications were continued at the same dosages. Over the next month, the severe bradycardia and hypotension resolved.
Discussion
The temporal correlation between quetiapine and the appearance of bradycardia and hypotension in our patient supported our suspician that quetiapine, possibly due to its higher dosage, directly contributed to the cardiac abnormalities seen in our patient.
Bradycardia has been reported as a severe adverse effect of SGAs such as risperidone, olanzapine, and clozapine. Though the precise mechanism that causes bradyarrhythmogenic characteristics in SGAs has not been fully elucidated, numerous studies have explored other adverse effects of SGAs, such as abnormal QT interval, interference with potassium ion transport to cardiac ventricular cells, and differences in medication distribution between the myocardium and plasma.[2] One study reported that most antipsychotic drugs block the human ether-à-go-go–related gene (hERG) and potassium and/or sodium ion channels (not as their therapeutic effect) and cause a concentration-dependent bradycardia in rat embryonic hearts.[3] Blockade of the potassium and/or sodium ion channels is manifested on ECG as QT prolongation and is sometimes associated with the potentially fatal conduction of torsade de pointes. Hypotension can be attributed to circulatory insufficiency due to severe bradycardia.
Quetiapine is a selective monoaminergic antagonist to dopaminergic (D2), serotoninergic (5-HT2A, 5-HT2C), histaminergic (H1), muscarinic (M1, M3), and adrenergic (a1,a2) receptors and a partial agonist to 5-HT1A receptors.[4] There are several hypotheses that attempt to explain receptor blockade effects. One hypothesis is that the central administration of 5-HT can cause bradycardia or tachycardia and hypo- or hypertension mediated by activation of 5-HT1A and 5-HT2 receptors. Another hypothesis suggests that alpha1-adrenegic antagonism with peripheral vasodilatation causes postural hypotension and compensatory tachycardia. We believe that the lack of beta-adrenergic affinity causes a sympatholytic effect that is exerted from the central instead of peripheral system. Since quetiapine possesses alpha2 affinity, this receptor up-regulation in the brain stem may induce bradycardia and hypotension at the same time.
Another point of consideration is that aging itself can contribute to an undesirably high concentration of quetiapine in the blood by decreasing hepatic activity of CYP3A4, which is the major metabolizing isoenzyme of quetiapine.[5]
Limitation. The relatively long amount of time (3 months) that passed between the final dosage escalation of quetiapine and the appearance of the cardiac symptoms in our patient limits our conclusion. Though we believe the higher dosage of quetiapine directly contributed to our patient’s cardiac symptoms, there were several other risk factors present in our patient that could have also contributed to his cardiac distress.
Conclusion
We suggest that clinicians remain vigilent for signs or symptoms of adverse effects in their elderly patients who take SGAs. Elderly patients with histories of heart failure, myocardial infarction, and/or conduction abnormalities may be particularly vulnerable to cardiac abnormalities while on quetiapine, particularly at higher dosages, and thus should be continually and closely monitored for any symptoms of cardiac distress.
References
1. Gareri P, De Fazio P, De Fazio S, et al. Adverse effects of atypical antipsychotics in the elderly: a review. Drugs Aging. 2006;23:937–956.
2. Nielsen J, Graff C, Kanters JK, et al. Assessing QT interval prolongation and its associated risks with antipsychotics. CNS Drugs. 2011;25:473–490.
3. Gunnström M1, Ababneh D, Webster WS, et al. Antipsychotic drugs cause bradycardia in GD 13 rat embryos in vitro. Reprod Toxicol. 2012;34:443–450.
4. Stahl SM. Antipsychotic agents. Essential Psychopharmacology. 3rd ed. Cambridge: University Press; 2008:327–451.
5. Sotaniemi EA, Arranto AJ, Pelkonen O, et al. Age and cytochrome P450-linked drug metabolism in humans: an analysis of 226 subjects with equal histopathologic conditions. Clin Pharmacol Ther. 1997;61:331–339.