
by Joan Busner, PhD; and Steven D. Targum, MD
Dr. Busner is Clinical Associate Professor of Psychiatry, Penn State College of Medicine, and Clinical Manager, United BioSource Corporation, Wayne, Pennsylvania; Dr. Targum is Consultant to Massachusetts General Hospital, Department of Psychiatry, Boston, Massachusetts
Disclosures: Dr. Busner has received grant support, served on the speaker bureau, or served as a consultant for the following pharmaceutical companies: Eli Lilly, Glaxo SmithKline, Bristol-Myers Squibb, Forest, Shire, and Merck. She is an employee of United BioSource Corporation; Dr. Targum is a consultant to the department of psychiatry at Massachusetts General Hospital, and has been a paid consultant to BrainCells Inc., Memory Pharmaceuticals, Prana Biotechnology, Epix Pharmaceuticals, Dynogen pharmaceuticals, Nupathe, United Biosource Corporation, and Johnson and Johnson PRD within the past year, and is an executive-in-residence at Oxford BioScience Partners (Boston, Mass.)
Key Words: Clinical Global Impressions Scale, quantification of patient outcome, tracking medication response, research tool for clinician
Abstract
Objective: This paper reviews the potential value in daily clinical practice of an easily applied research tool, the Clinical Global Impressions (CGI) Scale, for the nonresearcher clinician to quantify and track patient progress and treatment response over time. Method: The instrument is described and sample patient scenarios are provided with scoring rationales and a practical charting system. Conclusion: The CGI severity and improvement scales offer a readily understood, practical measurement tool that can easily be administered by a clinician in a busy clinical practice setting.
Introduction
The clinical reality is that most practicing psychiatrists/clinicians have multiple demands in busy practices with limited time to deliver excellent care, document the details, track response to interventions, and monitor and quantify patient progress. The 10-minute “med check” has become the norm across a wide variety of settings, dictated by large practice pressures and insurance reimbursement limitations. In that timeframe, the clinician attempts to assess, treat, and document care for a patient population that often presents with complex medical-psychiatric histories, multiple medication regimens, and complicated diagnostic pictures.
Validated psychiatric rating instruments are regularly employed by clinical researchers as the requisite basis for quantifying serial change during the course of clinical trials. Many of these clinician-rated instruments require specific ratings knowledge as well as available time to administer them. The obvious time constraints of real practice restrict their utility. Alternatively, the Clinical Global Impressions (CGI) scale is a well-established research rating tool applicable to all psychiatric disorders that can easily be used by the practicing clinician to meet this need.
In this paper, we review the administration of the CGI instrument and offer several scenarios to facilitate an understanding of the scoring rationale and practical value in assessing clinical progress in a busy clinical practice.
What is the CGI?
The CGI was developed for use in NIMH-sponsored clinical trials to provide a brief, stand-alone assessment of the clinician’s view of the patient’s global functioning prior to and after initiating a study medication.[1] The CGI provides an overall clinician-determined summary measure that takes into account all available information, including a knowledge of the patient’s history, psychosocial circumstances, symptoms, behavior, and the impact of the symptoms on the patient’s ability to function.
The CGI actually comprises two companion one-item measures evaluating the following: (a) severity of psychopathology from 1 to 7 and (b) change from the initiation of treatment on a similar seven-point scale. Subsequent to a clinical evaluation, the CGI form can be completed in less than a minute by an experienced rater. In practice, the CGI captures clinical impressions that transcend mere symptom checklists. It is readily understandable and can be used with relative ease by the non-researcher clinician. Beyond that, the CGI can track clinical progress across time and has been shown to correlate with longer, more tedious and time consuming rating instruments across a wide range of psychiatric diagnoses.
In clinical research, the CGI is administered by an experienced clinician who is familiar with the disease under study and the likely progression of treatment. Consequently, the CGI rater can make an expert clinical global judgment about the severity of the illness across various time points within the context of that clinical experience. The clinician makes a judgment about the total picture of the patient at each visit: the illness severity, the patient’s level of distress and other aspects of impairment, and the impact of the illness on functioning. The CGI is rated without regard to the clinician’s belief that any clinical changes are or are not due to medication and without consideration of the etiology of the symptoms.
Over the past 30 years, the CGI has been shown to correlate well with standard, well-known research drug efficacy scales (Hamilton Rating Scale for Depression, Hamilton Rating Scale for Anxiety, Positive and Negative Syndrome Scale, Leibowitz Social Anxiety Scale, Brief Psychiatric Rating Scale, Scale for the Assessment of Negative Symptoms, and others) across a wide range of psychiatric indications.[2–6] Although some revisions have been suggested,[7–10] the standard CGI is used in virtually all FDA-regulated and most other CNS trials. It is an instrument the non-researcher clinician can adapt with ease in a clinical setting; in fact, it is a clinical assessment—the only requirements for its use is that the scoring rationale is understood and that it is rated by a clinician who is experienced with the disease under study.
As noted above, the CGI has two components—the CGI-Severity, which rates illness severity, and the CGI-Improvement, which rates change from the initiation (baseline) of treatment.
CGI-Severity (CGI-S). The CGI-Severity (CGI-S) asks the clinician one question: “Considering your total clinical experience with this particular population, how mentally ill is the patient at this time?” which is rated on the following seven-point scale: 1=normal, not at all ill; 2=borderline mentally ill; 3=mildly ill; 4=moderately ill; 5=markedly ill; 6=severely ill; 7=among the most extremely ill patients.
This rating is based upon observed and reported symptoms, behavior, and function in the past seven days. Clearly, symptoms and behavior can fluctuate over a week; the score should reflect the average severity level across the seven days.
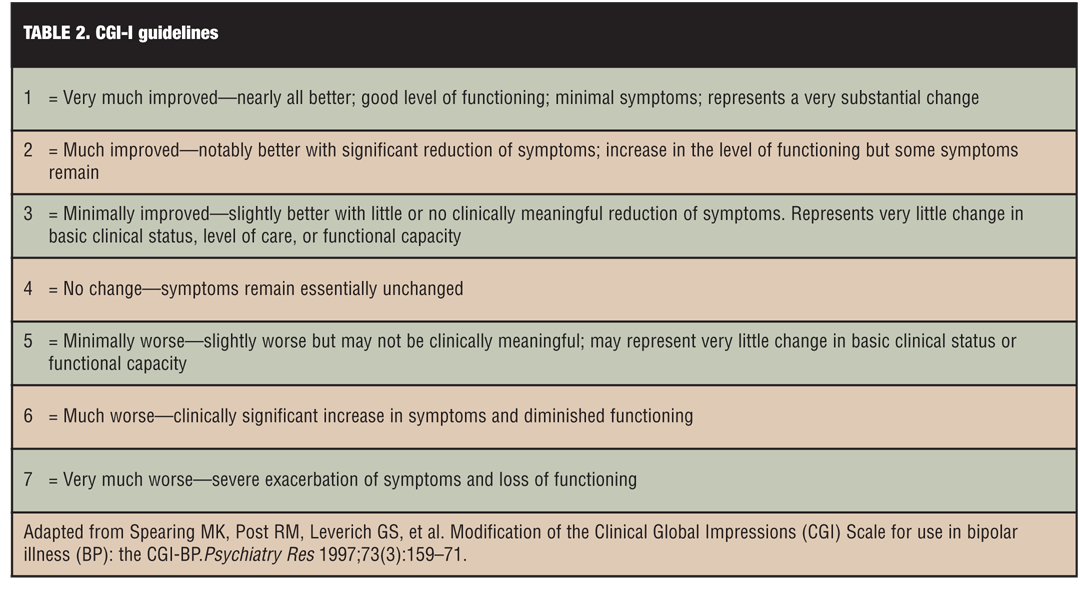
CGI-Improvement (CGI-I). The CGI-Improvement (CGI-I) is similarly simple in its format. Each time the patient is seen after medication has been initiated, the clinician compares the patient’s overall clinical condition to the one week period just prior to the initiation of medication use (the so-called baseline visit). The CGI-S score obtained at the baseline (initiation) visit serves as a good basis for making this assessment. Again, only the following one query is rated on a seven-point scale: “Compared to the patient’s condition at admission to the project [prior to medication initiation], this patient’s condition is: 1=very much improved since the initiation of treatment; 2=much improved; 3=minimally improved; 4=no change from baseline (the initiation of treatment); 5=minimally worse; 6= much worse; 7=very much worse since the initiation of treatment.”
The CGI-I score generally tracks with the CGI-S such that improvement in one follows the other. Anchors for scoring, however, are quite different, and the CGI-I is based upon changes from the initiation of treatment in contrast to changes from the preceding week of treatment. Consequently, the two CGI scores can occasionally be dissociated such that a clinician may notice changes in the CGI-I relative to baseline despite no recent changes in the overall CGI severity score or vice versa.
Can the CGI be used in clinical practice?
For researchers, the CGI has extraordinary utility. It is applicable across all CNS studies, including depression, schizophrenia, anxiety, no matter the population, drug, or other main study measures. It provides a readily recognizable and universally known efficacy measure that distinguishes it from the more complex, lengthier, and sometimes difficult to administer efficacy scales.
For the practicing clinician, the CGI has similar utility—it is quick to administer, it is applicable across all psychiatric disease states and all medications, it tracks for third parties (hospital or other institution, third party payers, pharmacy plan providers) progress and response, and it is a metric that documents due diligence on the part of the clinician to measure outcome. In some instances, the CGI measurement can be part of the clinical justification for off-formulary medications as medication non-response is often as important to document as medication response. The CGI allows the clinician to look back over the course of care and identify what interventions did or did not work. It allows even the busiest clinician to monitor patient progress in a consistent, systematic manner.
Administration of the CGI. Although there are no hard and fast rules for rating the CGI, general guidelines have evolved over the years. Some of the more commonly used conventions in research, along with illustrative scenarios, are provided.
Timeframe. The CGI is usually rated relative to the past seven days (including the day of the visit up to and through the visit). In this respect, the CGI is a state-dependent measure summarizing one week rather than a lifetime of symptoms and behavior.
Information sources. The CGI is designed to make use of all information available. Thus, a clinical interview with the patient should be combined with any other information available for the time period under study (past 7 days) from such sources as chart notes, family members, caseworkers, unit nurses, school teachers, for children, or significant others.
Questions to ask. To rate the CGI-S and the CGI-I, it is important to establish the presence of relevant symptoms, the frequency of their occurrence over the seven-day rating timeframe, the intensity or severity of the symptoms, and the effect of the symptoms on functioning in major areas of the patient’s life—work, home, school, and relationships.
CGI Scoring Guidelines
There are no universally accepted scoring guidelines for the seven anchor points; rather they were designed to be based solely on clinical judgment. Presented in Table 1 and Table 2 are some generically applicable guidelines based on severity and change guidelines used in clinical research and published for specific diseases. These guidelines have been modified for this paper for better applicability across diseases. The guidelines should be used as suggestions, not absolutes, for scoring. Clinical judgment and “gut” sense about the patient may warrant scoring the severity of illness as more or less severe, or the change from baseline as more or less improved, than the suggested guidelines would indicate.
CGI Scoring Examples
Following are some clinical scenarios that apply the typical conventions for scoring the CGI:
CGI-S Example 1. Depression. A 38-year-old, well-groomed, female patient, a successful litigation attorney, reports a one-month unprecipitated depressive episode that seems to be worsening. She is currently experiencing early morning awakening, loss of pleasure in her usual activities, feelings of guilt, reduced appetite, tearfulness, and depressed mood. She has found herself weeping several times over the past week, but cannot identify a reason. She is continuing to work, but found herself fighting back tears at an important meeting and believes her work may be less sharp than it had been in the past. No one has noticed, but she is concerned that the depression is worsening and may result in a significant impact on work. She is worried that she may lose her “edge.” She denies suicidal ideation. She has no previous psychiatric history.
Suggested CGI-S Score=4 (moderately ill)
Rationale: This patient has symptoms that are consistent with major depressive disorder and are beginning to affect her functioning. She might benefit from a medication treatment. These elements both suggest a score no less than a 4 (moderate). The patient’s functioning at a very demanding job is only affected to a limited degree at this point; no one has noticed and her lessened performance does not seem extreme. She continues to work her normal schedule. Although distressed, her illness has not caused a distinct impairment of occupational function that would raise the score to a 5 (markedly ill).
CGI-S Example 2. Schizophrenia. A 34-year-old, male patient with a diagnosis of paranoid schizophrenia has attended a partial hospitalization program off and on for 12 years. According to his caseworker, he had been stable on his medication regimen for the past year, but recently stopped taking his medication and would not cite a reason. He attended the partial program only one of the expected four days this past week and this was after the caseworker went to his home and drove him to the treatment facility. The caseworker reports he has become increasingly threatening and difficult to manage and has been seen responding to auditory hallucinations, including taking cover behind furniture in attempts to hide from “enemies.” In the past week, he obeyed a command hallucination to “go after” a fellow patient, but was physically circumvented from harming the patient by three staff members, who physically restrained him. The caseworker reported that although the patient was passively cooperative about coming to today’s visit, he did not speak with her at all during the trip. In the office, he is guarded and suspicious. He mumbles under his breath, but refuses to elaborate as to what he has said or to whom it was directed. Twice he makes a fist and raises his arm threateningly in the direction of the psychiatrist, but then puts his hand back in his lap. He appears disheveled and is ungroomed; he has not changed his clothing over the past week, which his caseworker reports is a new behavior for him.
Suggested CGI-S score=6 (severely ill)
Rationale: The patient’s functioning is clearly affected by his symptoms to the extent that he is not attending his day treatment program or taking his medication. Previously well groomed, he has now stopped even basic elements of self-care and hygiene. His behavior required restraint and may have posed a physical risk to others. This is a patient one might actively consider hospitalizing. Based upon his disruptive pathology and behavior influenced by symptoms (hallucinations), a CGI-S score of 6 (severely ill) is warranted. This patient did attend his day treatment program one day and did willingly accompany the caseworker to his visit with the psychiatrist, suggesting a somewhat lessened level of severity than a 7 would imply.
CGI-I Example 1. Anxiety. A patient who has been in treatment and receiving an SSRI for an anxiety disorder for four months comes in for a medication check. The patient’s CGI-S at the visit at which SSRI medication was initiated (“baseline” visit, to use clinical trial terminology) was 4 (moderate). At today’s visit, the patient reports that the anxiety symptoms have decreased considerably. The patient is now able to sleep 7 to 8 hours each night, with no initial insomnia. This represents a significant change from baseline, at which time the patient spent 2 to 3 hours each night trying to fall asleep, with a nightly total of 4 to 5 hours of fitful sleep. The patient reports having this week felt excessively anxious about running out of gas and about a burglar entering the house. The estimated time spent engaged in these anxious thoughts was less than one hour per day, compared to an estimated 3 to 4 hours per day at baseline. The patient drove over a bridge this week, which was described as somewhat difficult and fear-provoking, but manageable. At baseline, the subject was wholly avoidant of bridges, which caused him to drive 30 minutes out of his way each day to get to work.
Suggested CGI-I score=2 (much improved)
Rationale: The patient’s clinical status has clearly changed in the direction of improvement. For a CGI-I score of 3 (minimally improved), the level of change would not be sufficient to make an appreciable difference to the patient’s clinical status, level of distress, or functioning. This patient is now experiencing a significant nightly improvement in sleep, a reduction in time spent engaged in worry, and is driving over bridges allowing him to cut 60 minutes round trip off his daily commute. These improvements in distress level, symptom severity, and functional ability suggest an improvement score better than 3 because of his noticeable clinical improvement and better functioning. Nonetheless, the patient is still symptomatic; he endures the drive over the bridge with distress and still experiences anxious ruminations each day. Consequently, a rating of 2, much improved, rather than 1, very much improved, best captures this patient’s improvement relative to his baseline state.
CGI-I Example 2. Anxiety. The anxious patient in the previous example (CGI-I Example 1) returns one month later. He reports that he is now afraid of leaving his house without accompaniment. This is a new development for him. He is anxious and worried all day long. He called work and told them he had the flu. In reality, he was afraid to leave his house. He has only left the house three times this week, including his visit to the clinic today, all accompanied by his wife. He felt panicky on all three occasions. Although he denies any lightheadedness or other symptoms suggesting impending syncope, he reports worrying constantly about “passing out” in front of a moving car or bus. He is fearful that he will forget the name of a well-known friend or relative should they call him on the phone. He is sleeping only 1 to 2 hours a night. His wife reports that she has “never seen him so bad.” He cries in the interview and admits he has considered “ending it all” to make the pain go away.
Suggested CGI-I score=7 (very much worse)
Rationale. The patient has clearly worsened relative to his baseline condition. The patient has stopped going to work and is barely leaving his home. His worries are almost constant, clearly excessive, and are virtually all-consuming. The worries have become less reality-based and are a source of almost unendurable mental distress. He is barely sleeping. The patient finds his situation painful to the point of entertaining suicidal thoughts. Overall, the patient’s level of symptoms, frequency of symptoms, and its effect on his functioning are far above a CGI-I of 5, (minimally worse), or even 6, much worse. His clinical status, relative to baseline, reflects a severe exacerbation of symptoms with a loss of functioning suggesting a CGI-I score of 7 (very much worse). As the ultimate decision-maker, the clinician rater decides if the patient rates a 6 or a 7. What is most important is that ratings are consistent across time and across patients.
Questions, Issues and Tips
What if I’m treating the patient for more than one condition? How should I complete the CGI? In most clinical trials, the drug under study is being evaluated for one primary condition (for example, depression or generalized anxiety disorder). In those situations, the CGI is typically rated relevant only to that condition. In clinical care, in contrast, the physician may be treating several conditions at once. Outside of the research setting the CGI is the tool of the clinician. For the clinician, the questions are always the severity of the overall condition and whether the patient’s overall condition is improving, worsening, or staying the same. Therefore, an adaptation of the instrument we suggest the clinician adopt is to score the CGI as the entire picture (overall assessment) within the past week encompassing all targeted symptoms and conditions. Maintaining supplemental short notes of the areas that have responded best or that still need attention will be very helpful in guiding treatment decisions. The CGI charting system presented here is designed to provide a place to track the issue of multiple targeted symptoms.
What if the patient has a side effect from the medication? Should that be reflected on the CGI? Earlier versions of the CGI included a place for determining the risk benefit ratio of side effects to symptom relief. Current versions do not, and the CGI rating should not incorporate side effects. The CGI charting system presented here is designed to provide a place to note any dose-limiting or otherwise important side effects.
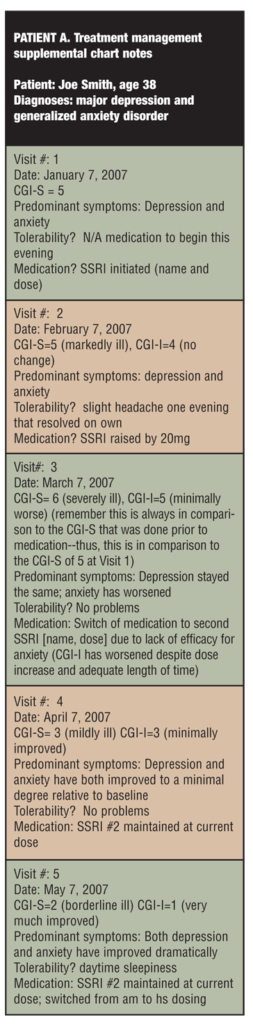
How would I use the CGI to help manage treatment? Although there are many possible systems a clinician might use to track CGI scores, a simple charting system that tracks visits with limited, concise amounts of supporting clinical data may be most useful. In this way, at a glance, the clinician is able to see the entire course of the patient’s treatment. Obviously, the clinician is free to track and chart any other areas of interest. The chart is presented in tabular form with sample supplemental chart notes. The tables should be used as a guide for setting up a template with abbreviated information (see Patients A and B Sample Tables and Chart Notes). The chart notes may be used to supplement the table. Complete the chart notes and table at the end of each patient visit and then move them up to the next visit so they remain a current running log.
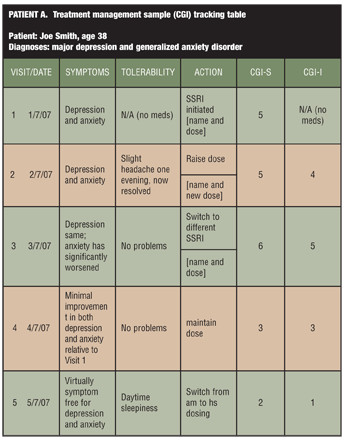
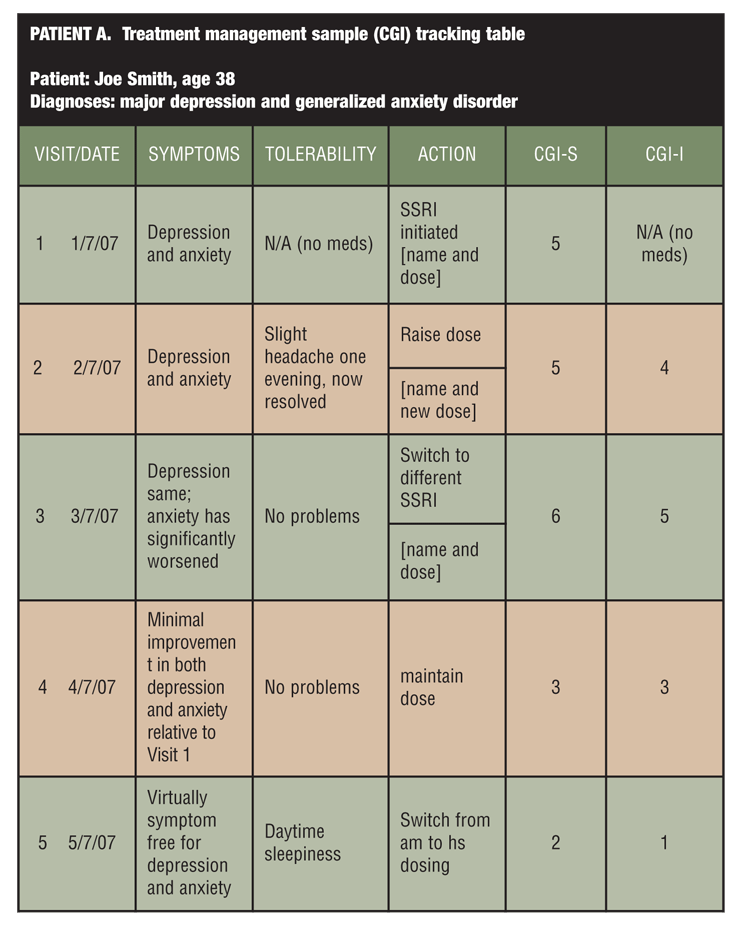
Discussion of Patient A. For the case described in Treatment Management Patient A (See Patient A tables below) the CGI chart can be used to track progress over time. By scanning the last 2 columns, it is apparent that this patient has improved from an initial severity of 5 (markedly ill) to a severity of 1 (normal, not at all ill) over the course of treatment. The patient’s improvement level on various interventions ranged from 5 (minimally worsened from visit 1) to 1 (very much improved) by the final treatment date shown. Details of the visits can be fleshed out in the accompanying chart notes format, as well as, of course, by traditional chart notes.
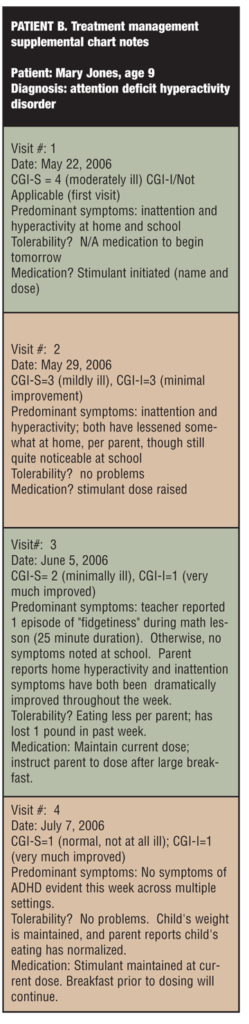
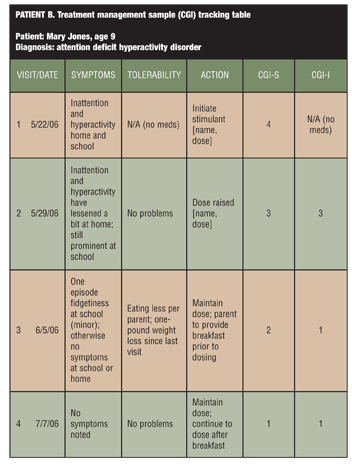
Discussion of Patient B. The case described in Treatment Management Patient B also illustrates the utility of the CGI chart in tracking treatment progress over time. The patient’s global assessment changes from a CGI-S of 4 (moderate) at Visit 1 to a CGI-S of 1 (normal, not at all ill) by Visit 4. Her CGI-I is rated as a 1 (very much improved) by Visit 3 although there are still some residual symptoms (subtle pathology). Her medication course, including tolerability issues and changes to doses, as well as other interventions (e.g., dosing after food) are also documented. Details of the visits can be fleshed out in the accompanying brief chart notes format, as well as, of course, by traditional chart notes.
At the patient’s next visit, the CGI tracking table and notes will be ready for quick perusal by the clinician.
Conclusions
The CGI can be a useful, easily adopted tool for the practicing clinician. It is a brief, understandable quantification method that can facilitate treatment over time.
References
1. Guy W (ed). ECDEU Assessment Manual for Psychopharmacology. Rockville, MD: US Department of Heath, Education, and Welfare Public Health Service Alcohol, Drug Abuse, and Mental Health Administration, 1976.
2. Bandelow B, Baldwin DS, Dolberg OT, et al. What is the threshold for symptomatic response and remission for major depressive disorder, panic disorder, social anxiety disorder, and generalized anxiety disorder? J Clin Psychiatry 2006;67:1428–34.
3. Leucht S, Kane JM, Kissling W, et al. Clinical implications of brief psychiatric rating scale scores. Br J Psychiatry 2005;187:366–71.
4. Leucht S, Engel RR. The relative sensitivity of the Clinical Global Impressions Scale in the Brief Psychiatric Rating Scale in antipsychotic drug trials. Neuropsychopharmacology 2006;31:406–12.
5. Spielmans GI, McFall JP. A comparative meta-analysis of Clinical Global Impressions change in antidepressant trials. J Nerv Ment Dis 2006;194:845–52.
6. Zaider TI, Heimberg RG, Fresco DM, et al. Evaluation of the Clinical Global Impression Scale among individuals with social anxiety disorder. Psychol Med 2003;33:611–22.
7. Beneke M, Rasmus W. Clinical Global Impressions (ECDEU) : Some critical comments. Pharmacopsychiatry 1992;25:171–6.
8. Haro JM, Kamath SA, Ochoa S, et al. The Clinical Global Impression-Schizophrenia Scale: A simple instrument to measure the diversity of symptoms present in schizophrenia. Acta Psychiatr Scand 2003;107(suppl 416):16–23.
9. Kadouri A, Corruble E, Falissard B. The improved Clinical Global Impression Scale (iCGI): Development and validation in depression. BMC Psychiatry 2007;7:7.
10. Spearing M, Post RM, Leverich GS, et al. Modification of the Clinical Global Impressions (CGI) Scale for use in bipolar illness (BP): The CGI-BP. Psychiatry Res 1997;73:159–71.