
Innov Clin Neurosci. 2026;23(4–6):51–55.
by Takahiko Nagamine, MD, PhD
Dr. Nagamine is with the Department of Psychiatric Internal Medicine, Sunlight Brain Research Center, Hofu, Japan and the Graduate School of Medical and Dental Sciences, Institute of Science Tokyo, Tokyo, Japan.
FUNDING: No funding was provided for this article.
DISCLOSURES: The author has no relevant conflicts of interest.
Schizophrenia is a severe and chronic mental illness for which pharmacological treatment remains the cornerstone of care. The primary therapeutic strategy involves the administration of psychotropic medications, particularly antipsychotics, aimed at managing the positive, negative, and cognitive symptoms of the disorder. However, these medications are frequently associated with severe adverse effects, including metabolic syndrome, extrapyramidal symptoms, and sedation, which can significantly impair quality of life and impede treatment adherence.1 This therapeutic gap has fueled a search for safer, more effective adjunctive treatments.
In recent years, considerable attention has been directed toward nutritional psychiatry, a field that explores the relationship between diet, nutrition, and mental health.2 The rationale for nutritional interventions in schizophrenia is twofold. First, individuals with schizophrenia often exhibit poor dietary patterns, characterized by high intake of processed foods and saturated fats and low intake of fruits, vegetables, and essential nutrients, which can be both a cause and a consequence of the illness.3 Second, emerging evidence suggests that nutritional factors play a pivotal role in the etiopathogenesis of schizophrenia, influencing neurodevelopment, neurotransmission, and inflammation.4 Several potential mechanisms link diet to the pathophysiology of schizophrenia. These include the role of B vitamins in 1-carbon metabolism essential for neurotransmitter synthesis, the pro-inflammatory potential of certain dietary patterns, and the intricate crosstalk between the gut microbiome and the central nervous system, often termed the microbiota-gut-brain axis (MGBA).5 However, despite a strong theoretical foundation and promising preliminary data, the clinical evidence remains fragmented and inconclusive. This narrative review aims to synthesize the current state of research on nutritional interventions for schizophrenia.
Methods
This narrative review aims to synthesize and critically evaluate the existing evidence on nutritional interventions for schizophrenia, focusing on 3 key mechanistic and therapeutic areas: 1-carbon metabolism and associated vitamin supplementation, the ketogenic diet, and interventions targeting the MGBA. The overarching goal is to provide a structured overview of the current landscape, elucidate the methodological challenges that impede clinical translation, and identify future research directions.
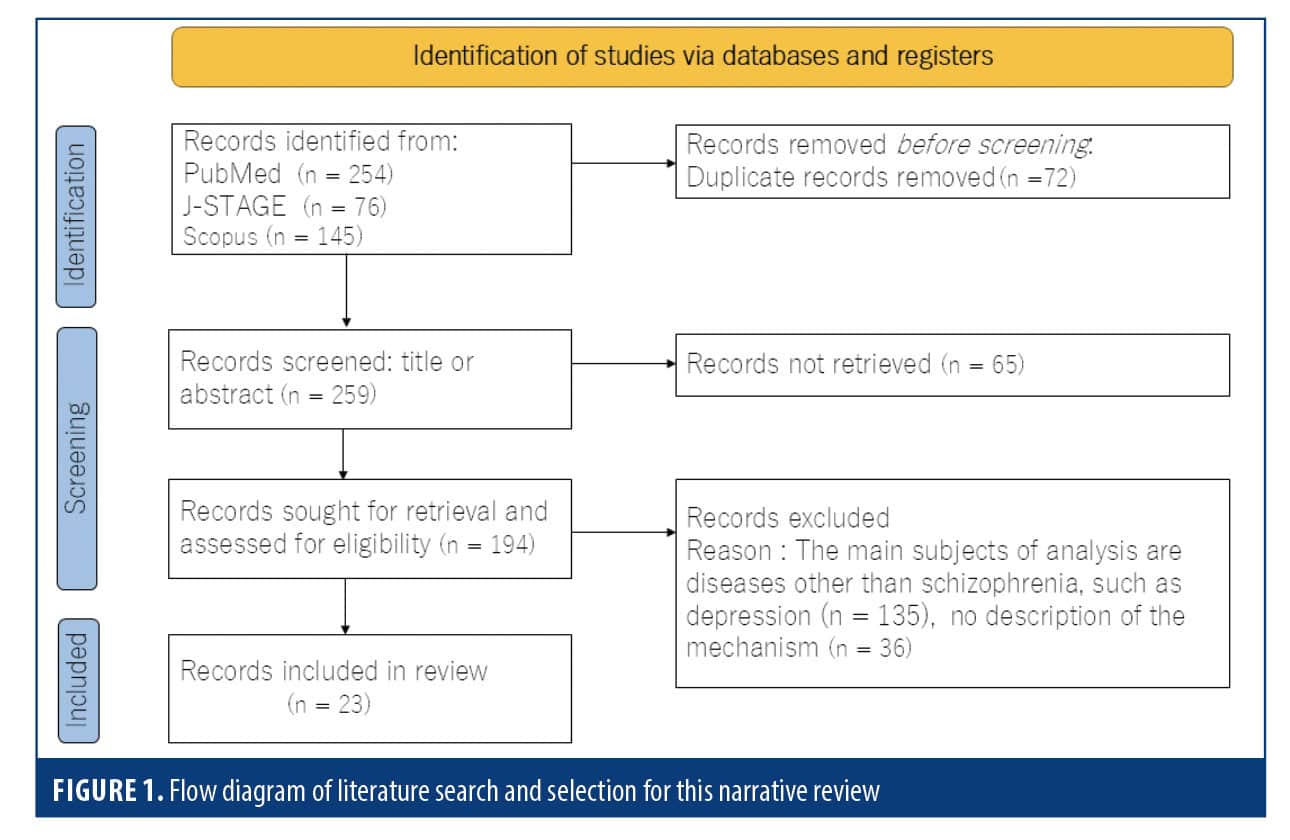
A comprehensive, albeit nonsystematic, search of the literature was conducted to identify relevant articles published between January 2014 and December 2024. The search was performed across 3 major electronic databases: PubMed, J-STAGE, and Scopus, chosen for their extensive coverage of biomedical and life sciences research. The search strategy employed a combination of keywords to capture a broad range of relevant studies. The core search terms included “schizophrenia” AND “nutritional intervention.” To specifically target the areas of focus for this review, this primary search was supplemented with more targeted searches using the following keyword combinations: (“schizophrenia” OR “psychosis”) AND (“vitamin B” OR “folate” OR “B12” OR “one-carbon metabolism”), (“schizophrenia” OR “psychosis”) AND (“ketogenic diet” OR “keto” OR “metabolic therapy”), and (“schizophrenia” OR “psychosis”) AND (“gut microbiota” OR “microbiome” OR “probiotics” OR “prebiotics”).
To ensure the contemporary relevance of the review, the search was limited to articles published in the last decade. The inclusion criteria were as follows: original research articles (including randomized controlled trials [RCTs], observational studies, and mechanistic studies), review articles, and meta-analyses; articles published in the English language; and studies focusing on human subjects with a diagnosis of schizophrenia or a related psychotic disorder. Preclinical and animal studies were considered for inclusion only when they provided crucial mechanistic insights directly relevant to the clinical literature being discussed. Exclusion criteria included editorials, letters to the editor, and case reports without substantial mechanistic discussion; studies where nutritional intervention was not a primary focus; and research pertaining to eating disorders or nutritional deficiencies unrelated to the core pathophysiology of schizophrenia. The selection of articles for inclusion was based on their relevance to the review’s aims, as determined by an initial screening of titles and abstracts, followed by a full-text review of potentially eligible papers. Given the narrative nature of this review, a purposive sampling approach was adopted to include seminal papers and studies that best illustrate the key concepts, findings, and challenges within each of the 3 focus areas. The process of the narrative review search is depicted in Figure 1.
Results
Vitamin status and supplementation outcomes. Observational studies have consistently identified nutritional deficiencies in individuals with schizophrenia. A substantial body of research indicates that, compared to healthy controls, patients with schizophrenia often present with lower serum levels of several vitamins critical for brain function. This includes notable deficiencies in B vitamins, such as folate (vitamin B9), vitamin B6, and vitamin B12, as well as in vitamin D.6 These findings from cross-sectional studies are robust, though the therapeutic impact of correcting these deficiencies remains a complex and evolving area of research.
A notable number of meta-analyses of observational studies have confirmed the association between schizophrenia and lower levels of key B vitamins.7 For folate, systematic reviews and meta-analyses have consistently demonstrated that individuals with schizophrenia have significantly lower serum and red blood cell folate concentrations compared to healthy individuals.8 This deficiency is noteworthy, as folate is essential for neurotransmitter synthesis and methylation processes in the brain. Similarly, a meta-analysis focusing on vitamin B6 found that serum pyridoxal levels, the active form of vitamin B6, were significantly decreased in patients with schizophrenia.9 The evidence for vitamin B12 deficiency is less uniform, with some studies indicating lower levels while others report no significant difference or even higher levels in certain patient populations.10
The prevalence of vitamin D deficiency in schizophrenia is particularly striking. A comprehensive meta-analysis revealed that 65% of individuals with schizophrenia had vitamin D deficiency.11 The mean difference in vitamin D levels between patients and controls was also significant, further underscoring the strong association between hypovitaminosis D and the disorder. Despite this well-established correlation between vitamin deficiencies and schizophrenia, results from clinical trials designed to correct these deficiencies have been inconsistent.12
Supplementation with these vitamins has not uniformly translated into significant clinical improvements, leading to a nuanced and sometimes contradictory body of evidence. For instance, meta-analyses of folic acid supplementation as an adjunctive treatment for schizophrenia have demonstrated only modest, if any, benefits.13 While some analyses suggest a small but statistically significant improvement in negative symptoms, such as apathy and social withdrawal, there is generally no effect observed on the overall, positive, or general symptoms of the disorder.14 The efficacy of folate supplementation might also be influenced by the patient’s genetic makeup, particularly variants in genes related to folate metabolism. Intervention trials using B vitamins, including vitamins B6 and B12, have also yielded mixed results.15 A meta-analysis of studies using high-dose B-vitamin supplementation (encompassing B6, B8, and B12) found a significant reduction in overall psychiatric symptoms compared to standard treatments alone.16 The review also suggested that supplementation might be more effective in the earlier stages of the illness. However, when analyzed individually, the effects on specific symptom domains, such as positive and negative symptoms, were not consistently significant.
Similarly, despite the strong observational link, intervention trials using vitamin D supplementation have not produced conclusive evidence to support its routine use for treating the core symptoms of schizophrenia. While crucial for overall health and bone density, which are also concerns in this patient population, the direct impact of vitamin D on psychosis remains an area of active investigation with currently insufficient support from RCTs to establish it as a standard treatment.17 A network meta-analysis comparing various nutritional supplements found that other agents, such as N-acetyl cysteine, might be more effective than B vitamins in improving overall symptom scores as measured by the Positive and Negative Syndrome Scale.18 This highlights the need for further research to identify which patient subgroups might benefit from specific nutritional interventions and to clarify the optimal dosages and treatment durations.
Ketogenic diet investigations. Research into the therapeutic potential of the ketogenic diet for schizophrenia is in its nascent stages, with the current evidence being primarily preclinical and preliminary. Preclinical evidence from animal models provides a foundational rationale for the diet’s proposed mechanism of action. In various rodent models designed to mimic schizophrenia-like behaviors, the ketogenic diet has been shown to normalize a range of abnormalities.19 For example, studies have demonstrated that the diet can reverse deficits in sensorimotor gating, a key endophenotype of schizophrenia, and attenuate hyperactivity induced by dopamine agonists. These animal studies also point toward underlying biological changes, including improvements in mitochondrial function, reduction in neuroinflammation, and modulation of neurotransmitter systems, particularly gamma-aminobutyric acid (GABA) and glutamate, which are thought to be dysregulated in schizophrenia.20
MGBA findings. Investigations into the MGBA in schizophrenia have yielded several key findings, primarily from comparative human studies and preclinical models.21 These results consistently point toward microbial dysbiosis in patients, and animal studies have begun to elucidate the potential pathophysiological roles of these microbes and the therapeutic potential of targeted interventions, such as probiotics and fecal microbiota transplantation (FMT).22
Comparative studies have revealed significant differences in the gut microbial composition of individuals with schizophrenia vs nonpsychiatric controls. A consistent finding across multiple studies and supported by meta-analyses is a reduction in microbial community richness and evenness, collectively known as alpha diversity.23 This indicates a less varied and potentially less resilient gut ecosystem in patients. Furthermore, specific alterations at the taxonomic level have been identified. While findings vary between studies, common observations include a decreased abundance of beneficial bacteria known to produce short-chain fatty acids (SCFAs), such as those from the genera Bifidobacterium and Lactobacillus, and butyrate-producing families, such as Lachnospiraceae and Ruminococcaceae.24 Conversely, an increased abundance of potentially pro-inflammatory taxa, such as those from the phylum Proteobacteria and certain species within the Clostridium genus, has been reported in some patient cohorts.29 These changes in microbial balance are often accompanied by measurable decreases in the fecal concentrations of key SCFAs, particularly butyrate, which is critical for maintaining gut barrier integrity and has known anti-inflammatory and neuroregulatory effects.29
The causal role of the gut microbiome in schizophrenia-related pathophysiology has been directly tested using FMT in animal models. In these experiments, germ-free mice, which are raised in a sterile environment and lack any microbiota, received fecal microbiota transplants from either individuals with schizophrenia or healthy controls.25 The mice that received FMT from individuals with schizophrenia subsequently developed behavioral abnormalities relevant to the disorder. These included psychomotor hyperactivity (a model for positive symptoms), deficits in cognitive functions such as working memory and spatial learning, and anxiety-like behaviors. These behavioral changes did not occur in mice colonized with microbiota from healthy donors.
Subsequent molecular analysis of the recipient mice revealed profound neurochemical alterations. The brains of mice colonized with a “schizophrenia microbiome” showed impaired tryptophan metabolism, a pathway critical for the synthesis of serotonin.26 Furthermore, these animals exhibited dysregulated dopamine, glutamate, and GABA systems in key brain regions implicated in schizophrenia, such as the hippocampus, striatum, and prefrontal cortex.27
Discussion
Interpreting the evidence: a gap between rationale and reality. The inconsistent outcomes of vitamin supplementation trials are particularly revealing of the challenges in this field. The robust observation of deficiencies, especially in B vitamins and vitamin D, creates a compelling, logical basis for supplementation. Yet, the fact that correcting a documented deficiency does not reliably or substantially improve the core symptoms of schizophrenia suggests that the relationship between nutrition and the disorder is not one of simple, unidirectional cause and effect. While poor nutrition, leading to these vitamin deficiencies, may certainly act as a risk factor, a potentiator of stress, or an exacerbating feature of the illness, the underlying pathophysiology of schizophrenia is likely far more complex than a simple nutrient deficit that can be easily reversed.28
The deficiencies themselves may be a consequence of the illness—driven by apathy, disorganized thinking, or poverty—or its treatment. For example, antipsychotic medications are known to alter metabolic processes and can interfere with nutrient absorption or utilization. Furthermore, associated lifestyle factors, such as higher rates of smoking, sedentary behavior, and limited access to fresh food, are powerful confounders.29 Therefore, while supplementation might be vital for the overall physical health of these individuals, its failure to consistently impact psychosis suggests the primary drivers of the illness lie deeper in neurodevelopmental and neurobiological processes that are not readily corrected by restoring nutrient levels in adulthood.
Regarding the ketogenic diet, the current evidence is hypothesis-generating at best and must be interpreted with significant caution. The positive signals from preclinical models, case reports, and a small pilot study are indeed encouraging, strongly suggesting that targeting cellular metabolism could be a viable and powerful strategy for a specific subset of patients, perhaps those with demonstrable mitochondrial dysfunction or glucose hypometabolism.30 However, enthusiasm must be tempered by the profound limitations of the current human evidence. Without adequately powered and controlled trials, it is impossible to disentangle true therapeutic effects from the potent influence of placebo responses, the impact of the intensive clinical support inherent in such studies, confounding variables such as weight loss, or the pervasive issue of publication bias, where positive findings are more likely to be reported. The significant commitment and potential risks required from patients to adhere to such a restrictive diet—which can impact social functioning, lipid profiles, and gut health—necessitate a much higher and more rigorous standard of evidence before it can be responsibly considered for any form of clinical recommendation.
The findings from MGBA research are perhaps the most mechanistically compelling, particularly the preclinical FMT studies. These experiments demonstrate a potential causal role for the gut microbiome in inducing schizophrenia-relevant behavioral and neurochemical phenotypes, shifting the paradigm from mere correlation to potential causation. However, extreme caution is essential when translating these striking results from highly controlled animal models to the complexities of human illness. The human microbiome is an incredibly complex and dynamic ecosystem, profoundly influenced by a host of factors, including long-term dietary patterns, geographical location, comorbid illnesses, and, critically in this population, chronic antipsychotic medication use, all of which are difficult to fully control for in clinical studies. While animal models provide powerful proof-of-concept studies, the specific microbial changes observed in human cross-sectional studies have been variable, and no single, universally accepted “schizophrenia microbiome” signature has been identified. This variability underscores the urgent need to move beyond identifying simple group-level differences and toward a more functional understanding of how an individual’s unique microbial ecology contributes to their illness, focusing on the metabolic output and inflammatory potential of the microbiome rather than just its composition.
Overarching methodological challenges in nutritional psychiatry. The difficulty in translating these promising preclinical and observational results into tangible clinical practice is largely a function of profound and unique methodological challenges. Nutritional science fundamentally differs from pharmacology in ways that stymie traditional research paradigms. A drug is typically a single molecule with a specific molecular target and predictable pharmacokinetics. In stark contrast, nutrition is a complex, multifaceted intervention with thousands of interacting components, whose effects are often diffuse, slow-acting, interactive, and highly dependent on the individual’s existing biological context. This inherent complexity makes it exceptionally difficult to study with the conventional research designs developed for pharmaceutical trials.
The gold-standard RCTs are particularly problematic in nutritional research. Effectively blinding a whole-diet intervention like the ketogenic diet is practically impossible, as participants are acutely aware of what they are eating. This introduces a significant risk of performance bias and makes it difficult to control for the powerful influence of expectancy and the placebo effect on mental health outcomes, which can be substantial. Furthermore, the long-term, cumulative impact of diet on brain structure and function is ill suited to the typically short duration of most RCTs, which may last only weeks or months. Such a timeframe is often insufficient to capture the slow cascade of biological changes, from altered gut function to shifts in neuroinflammation and synaptic plasticity, that are hypothesized to mediate the diet’s effects.31
While advanced statistical methods such as Mendelian randomization (MR) offer powerful tools for inferring causality from observational data by using genetic variants as proxies for exposure, its application in nutrition is also fraught with limitations. MR performs best when analyzing exposures with a clear, linear dose-response relationship. However, the biological effects of most nutrients often follow a nonlinear, U-shaped curve, where both deficiency and excess are detrimental. Standard MR analyses that fail to model this nonlinearity or account for the baseline nutritional status of participants are ill equipped to detect a true causal link and can lead to null findings even when a real effect exists at specific levels of intake.32
Future directions: a personalized, biomarker-guided approach. To overcome these formidable hurdles, the field of nutritional psychiatry must pivot from a one-size-fits-all approach to one of precision and personalization. The future of impactful research in this area lies not in testing broad dietary interventions on diagnostically heterogeneous patient populations, but in designing smarter, more targeted trials that are mechanistically informed by basic science. Future studies must be built on clear, testable mechanistic hypotheses and should incorporate a multiomics approach to stratify patients and rigorously measure biological responses. This strategy would involve integrating genomic data (eg, polygenic risk scores, genes for nutrient metabolism), microbiome profiles (both compositional and functional), metabolomics (to measure SCFAs and other products of microbial and host metabolism), and biomarkers of inflammation (eg, cytokines) and gut permeability (eg, zonulin).33
By leveraging artificial intelligence and machine learning algorithms to analyze these complex, high-dimensional datasets, researchers can move beyond simple group averages to identify robust biosignatures that predict which patients are most likely to benefit from a given nutritional strategy. For example, one could hypothesize that patients with a specific inflammatory profile and a gut microbiome poor in butyrate producers would be prime candidates for a trial of a fiber-enriched or ketogenic diet. Designing trials for these stratified, high-probability subgroups will dramatically increase the statistical power to detect a true therapeutic effect and pave the way for an evidence-based, personalized nutritional psychiatry that can be integrated into a holistic model of care for individuals with schizophrenia.34 This represents the most promising path to finally closing the gap between biological rationale and clinical reality.
Limitations. The conclusions presented in this narrative review should be considered in light of several important limitations. These limitations are inherent to the review’s methodology and the current state of the scientific literature on this topic. The foremost limitation is the nature of a narrative review itself. Unlike a systematic review, which adheres to a strict, predefined, and reproducible protocol (eg, Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines) to identify all available evidence, this review employed a purposive selection of literature. This approach, while effective for providing a thematic overview and discussing conceptual issues, is susceptible to selection bias. The author’s choice of which studies to include, emphasize, and synthesize is based on perceived relevance and impact, which introduces a degree of subjectivity that is not present in systematic methodologies. Consequently, this review is not exhaustive, and it is possible that other relevant studies have been omitted. Despite these limitations, this review serves its intended purpose: to provide a structured and critical overview of the current landscape, highlight key thematic areas of research, and discuss the conceptual and methodological challenges that must be addressed.
Conclusion
The current evidence for nutritional interventions in schizophrenia is more promissory than definitive, a situation born not from a lack of potential but from a profound mismatch between the complexity of nutrition and the conventional methods used to study it. The research to date strongly suggests that diet, metabolism, and gut health are deeply intertwined with the pathophysiology of schizophrenia, but this has not yet translated into effective, evidence-based clinical recommendations.
This gap does not signify that nutritional interventions are ineffective; rather, it underscores the urgent need for a paradigm shift in research methodology. Future progress hinges on our ability to move away from broad, population-level inquiries and toward personalized intervention trials. By leveraging biomarkers from genomics, metabolomics, and microbiome analysis, we can design more sophisticated studies that account for individual variability. The implementation of such controlled, biomarker-guided trials offers the most promising path to generating the high-quality evidence needed to finally establish the role of nutritional psychiatry in the holistic treatment of schizophrenia.
References
- MacKenzie NE, Kowalchuk C, Agarwal SM, et al. Antipsychotics, metabolic adverse effects, and cognitive function in schizophrenia. Front Psychiatry. 2018;9:622.
- Arroll MA, Wilder L, Neil J. Nutritional interventions for the adjunctive treatment of schizophrenia: a brief review. Nutr J. 2014;13:91.
- Teasdale SB, Ward PB, Samaras K, et al. Dietary intake of people with severe mental illness: systematic review and meta-analysis. Br J Psychiatry. 2019;214(5):251–259.
- Piper M, Beneyto M, Burne TH, et al. The neurodevelopmental hypothesis of schizophrenia: convergent clues from epidemiology and neuropathology. Psychiatr Clin North Am. 2012;35(3):571–584.
- Teasdale S, Mörkl S, Müller-Stierlin AS. Nutritional psychiatry in the treatment of psychotic disorders: current hypotheses and research challenges. Brain Behav Immun Health. 2020;5:100070.
- Cui X, McGrath JJ, Burne THJ, Eyles DW. Vitamin D and schizophrenia: 20 years on. Mol Psychiatry. 2021;26(7):2708–2720.
- Hiltensperger R, Neher J, Böhm L, Mueller-Stierlin AS. Mapping the scientific research on nutrition and mental health: a bibliometric analysis. Nutrients. 2025;17(3):399.
- Onaolapo OJ, Onaolapo AY. Nutrition, nutritional deficiencies, and schizophrenia: an association worthy of constant reassessment. World J Clin Cases. 2021;9(28):8295–8311.
- Tomioka Y, Numata S, Kinoshita M, et al. Decreased serum pyridoxal levels in schizophrenia: meta-analysis and Mendelian randomization analysis. J Psychiatry Neurosci. 2018;43(3):194–200.
- Campana M, Löhrs L, Strauß J, et al. Blood-brain barrier dysfunction and folate and vitamin B12 levels in first-episode schizophrenia-spectrum psychosis: a retrospective chart review. Eur Arch Psychiatry Clin Neurosci. 2023;273(8):1693–1701.
- Zhu JL, Luo WW, Cheng X, et al. Vitamin D deficiency and schizophrenia in adults: a systematic review and meta-analysis of observational studies. Psychiatry Res. 2020;288:112959.
- AlGhamdi SA. Effectiveness of vitamin D on neurological and mental disorders. Diseases. 2024;12(6):131.
- Sakuma K, Matsunaga S, Nomura I, et al. Folic acid/methylfolate for the treatment of psychopathology in schizophrenia: a systematic review and meta-analysis. Psychopharmacology (Berl). 2018;235(8):2303–2314.
- Allott K, McGorry PD, Yuen HP, et al. The vitamins in psychosis study: a randomized, double-blind, placebo-controlled trial of the effects of vitamins B12, B6, and folic acid on symptoms and neurocognition in first-episode psychosis. Biol Psychiatry. 2019;86(1):35–44.
- Roffman JL, Lamberti JS, Achtyes E, et al. Randomized multicenter investigation of folate plus vitamin B12 supplementation in schizophrenia. JAMA Psychiatry. 2013;70(5):481–489.
- Itokawa M, Miyashita M, Arai M, et al. Pyridoxamine: a novel treatment for schizophrenia with enhanced carbonyl stress. Psychiatry Clin Neurosci. 2018;72(1):35–44.
- Gaughran F, Stringer D, Wojewodka G, et al. Effect of vitamin D supplementation on outcomes in people with early psychosis: the DFEND randomized clinical trial. JAMA Netw Open. 2021;4(12):e2140858.
- Xu X, Shao G, Zhang X, et al. The efficacy of nutritional supplements for the adjunctive treatment of schizophrenia in adults: a systematic review and network meta-analysis. Psychiatry Res. 2022;311:114500.
- Kraeuter AK, Mashavave T, Suvarna A, et al. Effects of beta-hydroxybutyrate administration on MK-801-induced schizophrenia-like behaviour in mice. Psychopharmacology (Berl). 2020;237(5):1397–1405.
- Kraeuter AK, van den Buuse M, Sarnyai Z. Ketogenic diet prevents impaired prepulse inhibition of startle in an acute NMDA receptor hypofunction model of schizophrenia. Schizophr Res. 2019;206:244–250.
- Munawar N, Ahsan K, Muhammad K, et al. Hidden role of gut microbiome dysbiosis in schizophrenia: antipsychotics or psychobiotics as therapeutics? Int J Mol Sci. 2021;22(14):7671.
- Mosquera FEC, Guevara-Montoya MC, Serna-Ramirez V, Liscano Y. Neuroinflammation and schizophrenia: new therapeutic strategies through psychobiotics, nanotechnology, and artificial intelligence (AI). J Pers Med. 2024;14(4):391.
- Nguyen TT, Hathaway H, Kosciolek T, et al. Gut microbiome in serious mental illnesses: a systematic review and critical evaluation. Schizophr Res. 2021;234:24–40.
- Ju S, Shin Y, Han S, Kwon J, et al. The gut-brain axis in schizophrenia: the implications of the gut microbiome and SCFA production. Nutrients. 2023;15(20):4391.
- Zhu F, Guo R, Wang W, et al. Transplantation of microbiota from drug-free patients with schizophrenia causes schizophrenia-like abnormal behaviors and dysregulated kynurenine metabolism in mice. Mol Psychiatry. 2020;25(11):2905–2918.
- Kelly JR, Minuto C, Cryan JF, et al. The role of the gut microbiome in the development of schizophrenia. Schizophr Res. 2021;234:4–23.
- Balu DT, Li Y, Puhl MD, et al. Multiple risk pathways for schizophrenia converge in serine racemase knockout mice, a mouse model of NMDA receptor hypofunction. Proc Natl Acad Sci U S A. 2013;110(26):E2400–E2409.
- Adan RAH, van der Beek EM, Buitelaar JK, et al. Nutritional psychiatry: towards improving mental health by what you eat. Eur Neuropsychopharmacol. 2019;29(12):1321–1332.
- Firth J, Solmi M, Wootton RE, et al. A meta-review of “lifestyle psychiatry”: the role of exercise, smoking, diet and sleep in the prevention and treatment of mental disorders. World Psychiatry. 2020;19(3):
360–380. - Hsu FY, Liou JY, Tang FY, et al. Ketogenic diet consumption inhibited mitochondrial one-carbon metabolism. Int J Mol Sci. 2022;23(7):3650.
- Yassin LK, Nakhal MM, Alderei A, et al. Exploring the microbiota-gut-brain axis: impact on brain structure and function. Front Neuroanat. 2025;19:1504065.
- Carnegie R, Zheng J, Sallis HM, et al. Mendelian randomisation for nutritional psychiatry. Lancet Psychiatry. 2020;7(2):208–216.
- Misiak B, Pawlak E, Rembacz K, et al. Associations of gut microbiota alterations with clinical, metabolic, and immune-inflammatory characteristics of chronic schizophrenia. J Psychiatr Res. 2024;171:152–160.
- Hampel H, Gao P, Cummings J, et al. The foundation and architecture of precision medicine in neurology and psychiatry. Trends Neurosci. 2023;46(3):176–198.