
Innov Clin Neurosci. 2026;23(4–6):56–61.
by Alexandra R. Rola, PharmD; Jared R. Bagley, PhD; and Emily E. Leppien, PharmD, BCPS, BCPP
All authors are with the Binghamton University School of Pharmacy and Pharmaceutical Sciences, Johnson City, New York.
FUNDING: No funding was provided for this article.
DISCLOSURES: The authors have no relevant conflicts of interest.
Abstract: Objective: The objective of this study was to review the characteristics, efficacy, and safety of suzetrigine in the treatment of acute pain. Methods: Literature was identified using PubMed and clinicaltrials.gov. Search terms included suzetrigine, Journvax, and VX-548, with further limitation to those published in English. Articles selected for inclusion were trials evaluating the safety or efficacy of suzetrigine. Results: Suzetrigine was evaluated for the treatment of moderate-to-severe acute pain in 2 published phase 2 trials and in 3 unpublished phase 3 trials. All studies report a statistically significant reduction in pain scores. High-dose suzetrigine showed statistically and clinically significant pain reduction vs placebo in abdominoplasty 48.4 (95% confidence interval [CI]: 33.6–63.1; P<0.0001), and bunionectomy 29.3 (95% CI: 14.0–44.6; P=0.0002). Additional unpublished data support potential future use in additional pain indications. Suzetrigine was well tolerated, with pruritus, muscle spasm, constipation, and headache reported as the most common side effects. Suzetrigine is a promising nonopioid alternative for acute pain and is the first of a potential new class of analgesics. However, its comparative efficacy to standard analgesics has not been established, nor has its efficacy when used beyond 14 days. Conclusion: The recent United States Food and Drug Administration approval of suzetrigine introduces a novel class of analgesics; however, its clinical impact has yet to be defined. Keywords: VX-548, suzetrigine, Journavx, acute pain, postoperative pain
Introduction
Acute pain refers to the physiologic response to harmful stimuli, commonly following injury, surgery, or illness, and typically resolves within 30 days regardless of intervention.1 Inadequate management, however, might facilitate the transition to chronic pain, a major contributor to functional impairment and diminished quality of life. As such, effective assessment and treatment remain essential.
Current management favors a multimodal approach targeting distinct pain pathways.1 Nonpharmacologic therapies are recommended as adjuncts to medication.1,2 Available agents include nonsteroidal anti-inflammatory drugs (NSAIDs), acetaminophen, local anesthetics, gabapentinoids, skeletal muscle relaxants, N-methyl-D-aspartate (NMDA) receptor antagonists, and opioids.1–6 Despite these agents, there remains a need for safer, more effective alternatives.1,5
Common agents, such as NSAIDs and opioids, frequently produce off-target effects.4 Particularly, opioids carry significant risks including tolerance, dependence, and respiratory depression.4–6 Nevertheless, they remain the cornerstone of acute pain management, including postoperative care.6 Continued reliance on opioids underscores the limited availability of effective alternatives.
Emerging research has focused on voltage-gated sodium channels, notably NaV1.7 and NaV1.8.4,6 Suzetrigine (Journvax), a selective NaV1.8 inhibitor, is the first United States Food and Drug Administration (FDA)–approved sodium channel blocker for moderate-to-severe acute pain in adults.7 Its mechanism offers an alternative for patients who cannot tolerate NSAIDs or opioids. However, questions remain regarding long-term and consistent efficacy.4,6 This review summarizes the pharmacology, pharmacokinetics, efficacy, and safety of suzetrigine in acute pain management.
Data source and selection
A comprehensive literature search of PubMed and ClinicalTrials.gov was conducted using the terms suzetrigine, Journvax, and VX-548. English-language clinical trials, randomized controlled trials, review articles, and systematic reviews published through April 9, 2025, were included. References of relevant articles were reviewed to identify additional sources. Prescribing information and FDA press releases were manually retrieved. Independent searches by 2 authors yielded identical results.
Medicinal chemistry and pharmacology
Suzetrigine (VX-548) is a potent, selective NaV1.8 inhibitor involved in nociceptive signaling in peripheral sensory neurons.8 Structurally derived from a benzimidazole core, it features a trifluoromethyl-substituted tertiary alcohol and aromatic groups that enhance NaV1.8 affinity, selectivity, and metabolic stability.9 Suzetrigine demonstrates an IC₅₀ of approximately 0.27 nM for NaV1.8, indicating exceptional potency and selectivity over other sodium channel isoforms.4 Selectivity arises from binding to the second voltage-sensing domain (VSD2), stabilizing the channel’s closed state.4,9
Suzetrigine exhibits a unique state-dependent inhibition profile characterized by reverse use-dependence, with inhibition partially relieved during repetitive depolarizations. This reflects preferential binding to resting or closed states, in contrast to conventional sodium channel inhibitors, which favor open or inactivated states.9 This mechanism enables selective attenuation of pain signaling while sparing normal nerve conduction, thereby reducing off-target effects.1
Pharmacokinetics
Suzetrigine demonstrates favorable pharmacokinetics for oral administration.1 Moderate absorption has been observed, with peak concentrations reached at 3 hours fasting and 5 hours postprandially. Food does not significantly affect overall exposure.3 Steady-state is typically achieved within 3 days of twice-daily dosing, consistent with its elimination half-life of approximately 24 hours.4
The drug undergoes extensive hepatic metabolism via CYP3A, forming an active metabolite, M6-SUZ, which has one-third the potency and a longer half-life (about 33 hours), leading to accumulation at steady state.2,4,6 Elimination is primarily metabolic, with roughly equal excretion in urine and feces.3
Pharmacokinetics show minimal variability across age, sex, weight, or race. Mild-to-moderate hepatic impairment modestly increases exposure, while renal impairment has little effect due to limited renal clearance.3
Dosage and administration
Suzetrigine is initiated at 100 mg orally on an empty stomach, at least 1 hour before or 2 hours after food. Twelve hours after the initial dose, 50 mg is administered every 12 hours, regardless of food intake. Treatment should be continued only as long as necessary to meet therapeutic goals. Use beyond 14 days has not been studied.7
Drug interactions
Suzetrigine is metabolized hepatically via cytochrome P450 enzymes. Animal data suggest involvement of CYP3A2 and CYP2C11, corresponding to human CYP3A.1 Co-administration with potent CYP3A inhibitors (eg, clarithromycin, ketoconazole) is contraindicated. Use with strong CYP3A inducers or grapefruit products should be avoided. With moderate CYP3A inhibitors, dosing should be reduced to every 24 hours after the fifth dose. Although suzetrigine is a CYP3A inducer, the clinical significance remains unestablished.7
Efficacy
Suzetrigine has been approved by the FDA for the management of moderate-to-severe acute pain. Ongoing trials are evaluating its use in peripheral neuropathy and lumbosacral radiculopathy (LSR).8 Efficacy has been demonstrated in phase 2 and 3 trials, though published data are limited to phase 2 studies of acute pain and a single-arm phase 3 trial.5,10 Evidence for other pain indications is limited to unpublished manufacturer data.
Nociceptive moderate-to-severe acute pain. Approval of suzetrigine was based on 2 published phase 2 trials5 and 2 unpublished phase 3 trials.3,11Abdominoplasty and bunionectomy were used as models for soft-tissue and bone pain, respectively,5 both of which are considered standard for acute pain trials.2,5 Neither the phase 2 nor phase 3 trials directly compared suzetrigine to opioids or standard care. Hydrocodone-acetaminophen was included but not evaluated as a primary or secondary comparator.5,6
The phase 2 trials employed a proof-of-concept, double-dummy design assessing multiple doses of suzetrigine. The primary endpoint was the time-weighted sum of pain-intensity difference over 48 hours (SPID48), based on Numeric Pain Rating Scale (NPRS) scores. Patients were stratified by baseline pain, and secondary outcomes included 24-hour pain and percent reduction.5
In the bunionectomy trial, 274 adults (NPRS ≥4; baseline: 6.6–6.9) were randomized to high-, middle-, or low-dose suzetrigine, hydrocodone-acetaminophen, or placebo (Table 1). In the abdominoplasty trial, 303 patients (baseline NPRS: 7.2–7.4) received high- or middle-dose suzetrigine, hydrocodone-acetaminophen, or placebo (Table 1). Fentanyl was allowed prerandomization; ibuprofen was available as rescue therapy.5 In both trials, analgesic response among the low-dose, middle-dose, hydrocodone-acetaminophen, and placebo groups was similar. Completion rates were high across studies (90.1% bunionectomy vs 81.5% abdominoplasty). Only high-dose suzetrigine significantly reduced pain vs placebo (bunionectomy, least-square means [LSM]: 36.8; 95% confidence interval [CI]: 4.6–69.0; abdominoplasty, LSM: 37.8; 95% CI: 9.2–66.4).5
An additional, phase 3 post-hoc analysis indirectly examined suzetrigine monotherapy vs multimodal use with ibuprofen to explore the potential of suzetrigine monotherapy. Each agent was compared to placebo. In abdominoplasty, least-squares mean difference in time-weighted sum of the pain intensity difference from 0 to 48 hours (SPID48) from placebo were 48.4 (95% CI: 33.6–63.1; P<0.0001) with and 47.7 (95% CI: 32.4–62.9; P<0.0001) without ibuprofen as rescue imputation, respectively. In bunionectomy, LSM difference form placebo were 29.3 (95% CI: 14.0–44.6; P=0.0002) with and 28.8 (95% CI: 12.9–44.6; P=0.0004) without ibuprofen, supporting monotherapy.12
Subsequent phase 3 trials built on these findings. Pain-intensity difference from baseline to 48 hours was the primary endpoint, comparing high-dose suzetrigine to placebo. A secondary analysis compared suzetrigine to hydrocodone-acetaminophen. Inclusion criteria expanded to patients aged 18 to 80 years with NPRS ≥4.11 Patients undergoing abdominoplasty or bunionectomy were randomized to high-dose suzetrigine, hydrocodone-acetaminophen, or placebo (Table 1).3,4 High-dose suzetrigine showed statistically and clinically significant pain reduction vs placebo: abdominoplasty 48.4 (95% CI: 33.6–63.1; P<0.0001), bunionectomy 29.3 (95% CI: 14.0–44.6; P=0.0002).11 Rapid and sustained relief was observed within a median time of 2 hours for abdominoplasty (P<0.0001) and 4 hours for bunionectomy (P=0.0016) with suzetrigine, compared to 8 hours for both surgeries with placebo. At 48 hours, changes from baseline in NPRS were comparable between suzetrigine and hydrocodone bitartrate-acetaminophen (abdominoplasty: –3.4 vs –3.2; bunionectomy: –3.4 vs. –3.6).3,11,13 No significant difference was seen in abdominoplasty (LSM difference: 6.6; 95% CI: –5.4 to 18.7; P=0.2781),11 though bunionectomy favored suzetrigine (LSM difference: –20.2; 95% CI: –32.7 to –7.7; P=0.0016).11
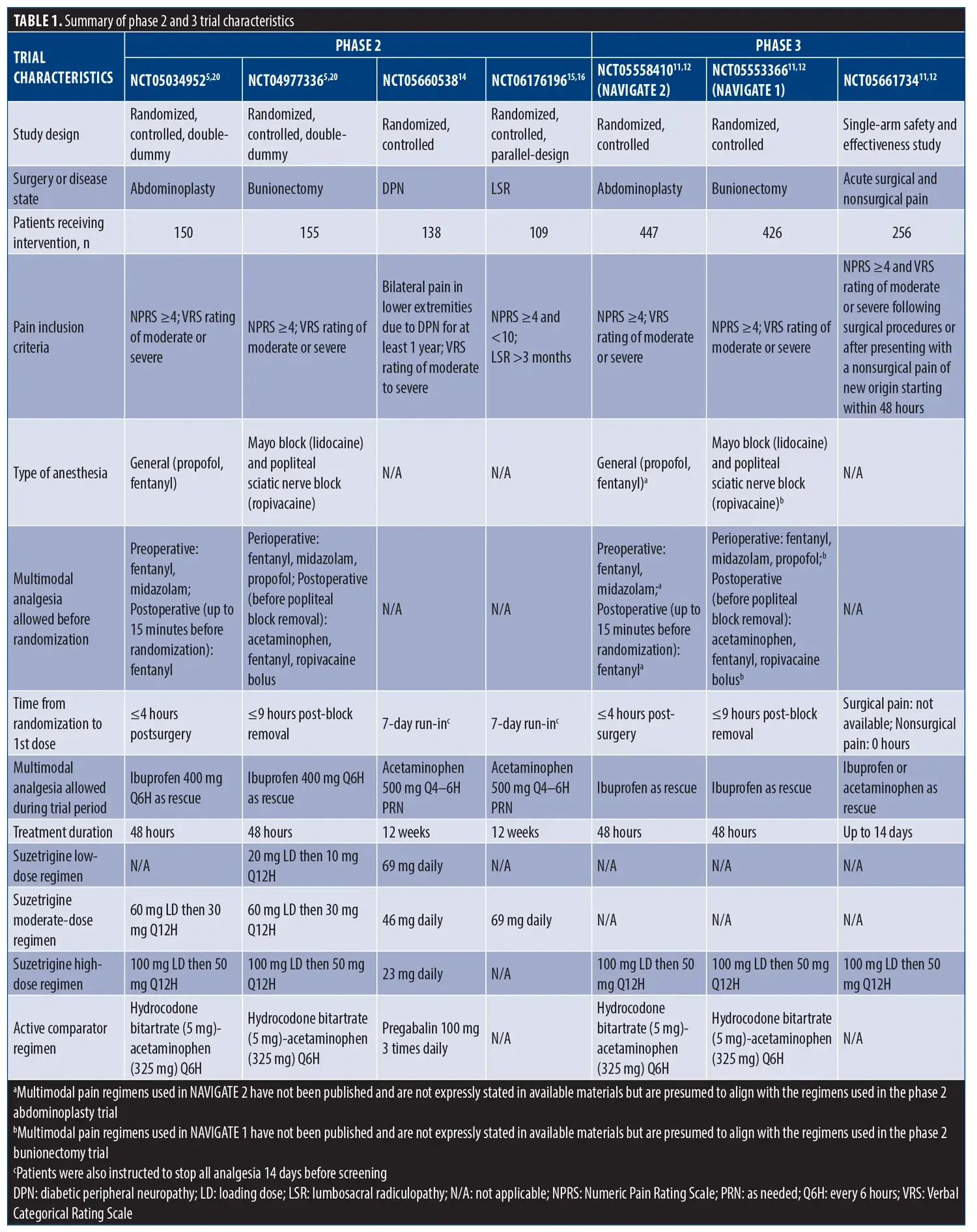
A single-arm phase 3 trial evaluated 14-day use of high-dose suzetrigine for moderate to severe acute pain in 256 patients (NPRS ≥4). Acetaminophen or ibuprofen was allowed as rescue therapy.4,10–12 Efficacy was consistent across pain types, with 82.0% of surgical and 91.2% of nonsurgical patients reporting at least good pain control.10
Diabetic peripheral neuropathy. A phase 2 proof-of-concept trial was conducted to evaluate suzetrigine for diabetic peripheral neuropathy (DPN). Although unpublished, results were released by the manufacturer. The primary endpoint was a clinically meaningful reduction in average pain over 12 weeks. Following a 14-day washout, 164 patients were randomized 2:1:2:2 to receive pregabalin 100 mg 3 times daily or suzetrigine 23, 46, or 69 mg daily. Sustained pain reduction was observed across all groups, with the greatest reduction in the suzetrigine 69 mg group (–2.18; 95% CI: –2.94 to –1.41; P<0.0001). Over 30% of suzetrigine-treated patients achieved ≥50% pain reduction, and 20% receiving 46 or 69 mg achieved >70% reduction.14 A phase 3 trial is currently enrolling (NCT06696443).
LSR. An unpublished phase 2 proof-of-concept trial evaluated suzetrigine for LSR over 12 weeks. Adults aged 18 to 70 years with LSR for ≥3 months and baseline pain scores between 4 and 10 were randomized to receive suzetrigine 69 mg daily or placebo. Although a clinically significant reduction in leg pain was observed, the treatment curves did not separate (suzetrigine: –2.02; placebo: –1.98), indicating no benefit over placebo. Post-hoc analysis attributed this to a substantial placebo effect. Greater separation was observed at sites without pronounced placebo responses.15,16
Safety
Limited safety data suggest that suzetrigine is well tolerated with short-term use. The most common adverse effects (AEs) include pruritus, muscle spasm, elevated creatine phosphokinase, and rash.7 In phase 2 trials, nausea, vomiting, headache, constipation, and dizziness occurred in >10% of patients, though only constipation and headache were more frequent with suzetrigine. Most AEs were mild and self-limited, with no serious events attributed to the drug and no significant lab, vital sign, or electrocardiogram changes.3,5
In phase 2 trials for DPN and LSR, suzetrigine was well tolerated, with a low incidence of AEs.14–16 In the DPN trial, AEs occurred in 14.7% of suzetrigine-treated patients compared to 27.8% with pregabalin.14 Higher rates were observed in the LSR trial, with 22.9% of suzetrigine-treated patients reporting AEs.15,16
In phase 3 abdominoplasty and bunionectomy trials, AEs were mild to moderate, occurring comparable rates in the suzetrigine and placebo arms, at 50.0% vs. 56.3% following abdominoplasty trial and 31.0% vs. 35.2% following bunionectomy.11 In the single-arm phase 3 trial, only mild-to-moderate events were reported, with headache being most common (36.7%).11,12 Discontinuation due to AEs occurred in 2% of patients.5,12
Suzetrigine’s safety advantage over opioids is supported by its peripheral NaV1.8 selectivity, minimizing central nervous system effects.1,5,6,8 No evidence of respiratory depression, sedation, dependence, or addiction has been reported.4,5 A pooled safety analysis (n=2,447) showed low abuse-related events, comparable to placebo. Dizziness was most common (3.8% suzetrigine vs. 6.4% placebo, 5.3% hydrocodone-acetaminophen), with other symptoms occurring in less than 2 patients per group.4
Cardiovascular risk, though hypothesized due to NaV1.8 expression and lidocaine analogies, has not been observed in trials.5,6,10,11,13 However, given the short trial durations and the low incidence of cardiovascular events with lidocaine, further data are needed to clarify potential risk.
Special populations
Limited data is available on suzetrigine’s use in special populations. Suzetrigine has not been studied in pediatric populations, and should be avoided in individuals under 18 years of age. Older adults, up to 80 years of age, were included in clinical trials,5,11 with no significant differences observed in those aged 65 to 75 years.5 However, full results from phase 3 studies involving patients up to 80 years of age are not yet available.11
Use of suzetrigine is not recommended in patients with severe hepatic impairment (Child-Pugh Class C) due to increased risk of AEs. In moderate hepatic impairment (Child-Pugh Class B), a reduced dosing regimen is required. Standard dosing is used through the fifth dose, then should be reduced to once daily.7
Limited data support the safety of suzetrigine in patients with an estimated glomerular filtration rate (eGFR) >15 mL/minute, and standard dosing is recommended. Use in patients with eGFR <15 mL/minute, or those receiving renal replacement therapy, has not been studied and should be avoided.7
Suzetrigine’s safety in pregnancy and lactation has not been established. Animal studies did not show malformations, birth defects, or miscarriage following oral administration during gestation; however, relevance to human development remains unknown.7
Data suggest that suzetrigine might temporarily reduce fertility in female individuals of childbearing age, based on findings in rats, though this effect has not been confirmed in humans.7 Potential interactions with hormonal contraceptives might reduce contraceptive efficacy during treatment and for 28 days after discontinuation. Nonhormonal back-up methods should be used in patients on hormonal contraceptives. Use during pregnancy should be avoided.7,11
Safety of breastfeeding with suzetrigine is unknown. While it is not known whether suzetrigine is excreted in human milk,11 it has been detected in animal milk, suggesting potential exposure.7
Access and financial considerations
Cost remains a barrier to suzetrigine use, as it is more expensive than generic analgesics. The average tablet cost is approximately $18, with typical dosing requiring 2 to 3 tablets daily.17 Patient assistance and copay programs are currently offered by the manufacturer to improve access. While initial costs can be high, long-term savings might be seen if suzetrigine reduces opioid use and associated complications.18
Place in therapy
Suzetrigine represents a promising nonopioid option for acute pain management; however, its comparative efficacy to standard analgesics has not been established. In clinical trials, suzetrigine was evaluated against conservative NSAID and opioid regimens, limiting applicability in settings requiring higher opioid doses or patient-controlled analgesia.18 Given its unique mechanism targeting peripheral nociceptive neurons, suzetrigine might offer utility in patients unable to tolerate or safely use other agents, including those with or at risk for substance use disorders—though supporting evidence is currently lacking.1,2,6,12 While suzetrigine has demonstrated fewer AEs compared to alternatives, its short duration of use limits its role in clinical practice. Its high cost also restricts widespread adoption.19 Enthusiasm for suzetrigine’s role should be tempered, with use guided by individual patient characteristics.
Conclusions
While suzetrigine introduces a novel class of analgesics, further studies are required to establish its role in clinical practice and expanded indications. Current approval for short-term treatment of moderate-to-severe acute pain is based on its reduced risk of tolerance and dependence. However, evidence does not support opioid replacement, as long-term efficacy and safety remain undetermined. Additional research is needed to evaluate its use within multimodal regimens. Although suzetrigine could serve as an adjunct or alternative to opioids, its clinical impact has yet to be defined.
References
- Oliver B, Devitt C, Park G, et al. Drugs in development to manage acute pain. Drugs. 2025;85(1):11–19.
- Kaye AD, Greene DR, Nguyen C, et al. Emerging medications and strategies in acute pain management: evolving role of novel sodium and calcium channel blockers, peptide-based pharmacologic drugs, and non-medicinal methods. Curr Pain Headache Rep. 2024;28(9):853–862.
- Hang Kong AY, Tan HS, Habib AS. VX-548 in the treatment of acute pain. Pain Manag. 2024;14(9):477–486.
- Osteen JD, Immani S, Tapley TL, et al. Pharmacology and mechanism of action of suzetrigine, a potent and selective NaV1.8 pain signal inhibitor for the treatment of moderate to severe pain. Pain Ther. 2025;14:655–674.
- Jones J, Correll DJ, Lechner SM, et al. Selective inhibition of NaV1.8 with VX-548 for acute pain. N Engl J Med. 2023;389(5):393–405.
- Kaye AD, Everett ES, Lehuquet AM, et al. Frontiers in acute pain management: emerging concepts in pain pathways and the role of VX-548 as a novel NaV1.8 inhibitor: a narrative review. Curr Pain Headache Rep. 2024;28(11):1135–1143.
- Journavx. Prescribing information. Vertex Pharmaceuticals Inc.; revised Jan 2025. Accessed 6 May 2026. https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/219209s000lbl.pdf
- Wang H, Huang J, Zang J, et al. Drug discovery targeting Nav1.8: structural insights and therapeutic potential. Curr Opin Chem Biol. 2024;83:102538.
- Vaelli P, Fujita A, Jo S, et al. State-dependent inhibition of Nav1.8 sodium channels by VX-150 and VX-548. Mol Pharmacol. 2024;106(6):298-308.
- McCoun J, Winkle P, Solanki D, et al. Suzetrigine, a non-opioid NaV1.8 inhibitor with broad applicability for moderate-to-severe acute pain: a phase 3 single-arm study for surgical or non-surgical acute pain. J Pain Res. 2025;18:1569–1576.
- Vertex announces positive results from the VX-548 phase 3 program for the treatment of moderate-to-severe acute pain. Vertex Pharmaceuticals Inc. 30 Jan 2024. Accessed 6 May 2026. https://investors.vrtx.com/news-releases/news-release-details/vertex-announces-positive-results-vx-548-phase-3-program
- Suzetrigine (VX-548) ASA update. Vertex Pharmaceuticals Inc. 20 Oct 2024. Accessed 26 May 2026. https://investors.vrtx.com/static-files/39514f75-f903-4a34-a729-7b1646b4b0f9
- Vx-548 phase 3 results in acute pain. Vertex Pharmaceuticals Inc. 30 Jan 2024. https://investors.vrtx.com/static-files/2b8b5989-a5ff-456a-8bf7-1709028d5f20
- VX-548 phase 2 results in painful diabetic peripheral neuropathy. Vertex Pharmaceuticals Inc. 13 Dec 2023. Accessed 6 May 2026. https://investors.vrtx.com/static-files/1eeed94f-d3fe-42f6-9557-2e71475afc35
- Vertex announces results from phase 2 study of suzetrigine for the treatment of painful lumbosacral radiculopathy. Vertex Pharmaceuticals Inc. 19 Dec 2024. Accessed 6 May 2026. https://news.vrtx.com/news-releases/news-release-details/vertex-announces-results-phase-2-study-suzetrigine-treatment
- Suzetrigine (VX-548) phase 2 results in painful lumbosacral radiculopathy. Vertex Pharmaceuticals Inc. 19 Dec 2024. https://investors.vrtx.com/static-files/0149bf23-3d32-41b5-8ca8-ec22c65f968d
- RED BOOK search – MICROMEDEX. Accessed 18 Jun 2025. https://www.micromedexsolutions.com.
- Rind DM, Nikitin D, Lee W, et al. Suzetrigine for acute pain: effectiveness and value; draft evidence report. Institute for Clinical and Economic Review. 9 Dec 2024. Accessed 18 Jun 2025.https://icer.org/wp-content/uploads/2024/12/ICER_Acute-Pain_Draft-Report_For-Publication_120924.pdf
- Kingwell K. NaV1.8 inhibitor poised to provide opioid-free pain relief. Nat Rev Drug Discov. 2024;24(1):3–5.
- A study evaluating efficacy and safety of VX-548 for acute pain after an abdominoplasty (NCT05034952). ClinicalTrials.gov. Updated 27 Dec 2024. Accessed 6 May 2026. https://clinicaltrials.gov/study/NCT05034952
- A study evaluating efficacy and safety of VX-548 for acute pain after a bunionectomy (NCT04977336). ClinicalTrials.gov. Updated 25 Jun 2025. Accessed 6 May 2026. https://clinicaltrials.gov/study/NCT04977336
- Evaluation of efficacy of safety of VX-548 for painful diabetic peripheral neuropathy (DPN) (NCT05660538). ClinicalTrials.gov. Updated 1 Jul 2025. Accessed 6 May 2026. https://clinicaltrials.gov/study/NCT05660538
- Evaluation of efficacy and safety of VX-548 for painful lumbosacral radiculopathy (PLSR) (NCT06176196). ClinicalTrials.gov. Updated 1 Oct 2025. Accessed 6 May 2026. https://clinicaltrials.gov/study/NCT06176196
- Evaluation of efficacy and safety of VX-548 for acute pain after abdominoplasty (NCT05558410). ClinicalTrials.gov. Updated 1 Jul 2025. Accessed 6 May 2026. https://clinicaltrials.gov/study/NCT05558410
- Evaluation of efficacy and safety of VX-548 for acute pain after a bunionectomy (NCT05553366). ClinicalTrials.gov. Updated 1 Aug 2025. Accessed 6 May 2026. https://clinicaltrials.gov/study/NCT05553366
- A single-arm study to evaluate safety and effectiveness of VX-548 for acute pain (NCT05661734). ClinicalTrials.gov. Updated 1 Jul 2025. Accessed 6 May 2026. https://clinicaltrials.gov/study/NCT05661734