

by Peta Stapleton, PhD; Dawson Church, PhD; Oliver Baumann, PhD; and Debbie Sabot, BA, Grad Dip Psych
Drs. Stapleton and Baumann and Ms. Sabot are with the School of Psychology, Bond University in Gold Coast, Queensland, Australia. Dr. Church is with the National Institute for Integrative Healthcare in Fulton, California.
Funding: Funding was provided by the National Institute for Integrative Healthcare.
Disclosures: Dr. Church may be renumerated for keynote presentations on this topic due to expertise. All other authors have no conflicts of interest relevant to the content of this article.
Innov Clin Neurosci. 2022;19(7–9):61–70.
Abstract
Background: The tendency of the mind to wander, a characteristic of the brain’s default mode network (DMN), correlates with increased unhappiness and self-referential processing and is a deterrent to establishing a consistent meditation practice. The objective of this study was to test the impact of a secular physiological method of meditation. We hypothesized that EcoMeditation would produce increases in neural communication in brain regions associated with compassion and prosociality and decreases in self-referencing networks, such as the DMN, and that these changes would be found in the experimental group, but not the control group.
Methods: Participants (n=38) were randomized into two groups, and the final sample consisted of 25 participants. One group listened daily to a 22-minute EcoMeditation audio track, while the other used an active control. Functional magnetic resonance imaging (fMRI) was used to assess brain function before and after four weeks of practice. Mystical experiences, as well as psychological conditions, such as anxiety and depression, were measured.
Results: Participants in the EcoMeditation group showed significantly increased connectivity between the bilateral hippocampus and the bilateral insula, compared to pre-intervention. In addition, significant decreases of connectivity between the bilateral hippocampus and the midprefrontal and left dorsolateral prefrontal cortices occurred. EcoMeditation participants also scored significantly higher for mystical experiences than the control group. The results for emotional states were mixed, with one assessment finding increased positive mood, but another finding increased negative affect.
Conclusion: After only four weeks, participants using EcoMeditation demonstrated brain states similar to meditation adepts with thousands of hours of traditional practice.
Keywords: Meditation, brain, EcoMeditation, functional magnetic resonance imaging
While meditation is an ancient spiritual practice, modern research methods have rendered it amenable to empirical investigation. Over the past 20 years, the literature on meditation has grown exponentially. In 1990, about 500 studies had been published. A current search shows over 5,000 studies in mainstream journals (found in the United States [US] National Library of Medicine and PubMed). This literature has led to an increased understanding of the therapeutic value of meditation, as well as an increase in mapping the neurophysiological changes associated with the practice.
Self-transcendent brain states. This increase in literature has, in turn, accelerated the translation of this research into clinically useful interventions.1–8 One form of meditation, mindfulness-based stress reduction (MBSR), has been shown to be effective for substance abuse,10–12 managing pain,13,14 and improving mood.15–16 Systematic reviews reveal that structured meditation interventions both reduce stress and increase psychological health when compared to active controls.15,17,18
A greater understanding of the psychological benefits of meditation has led to the investigation of its effects on the brain and nervous system. This new field, termed contemplative neuroscience, has been augmented by studies showing that meditation improves brain functions, such as attention, perception, and cognitive functions, which include decision-making and self-regulation.19–21 Other physiological benefits include improvements in biological markers of aging, immunity, and inflammation.1,22–24
Contemplative traditions also detail the phenomenology of self-transcendent altered states of consciousness.25–28 Practitioners describe experiences of “awakening” or “enlightenment,” sensations of transcending the physical body, a renewed sense of life purpose, and feelings of unity with the universe.29 A framework for defining the neural and behavioral characteristics of meditation, termed self-awareness, self-regulation, and self-transcendence (S-ART), has been proposed.30 This model defines self-transcendence as “a positive relationship between self and other that transcends self-focused needs and increases pro-social characteristics.”30 Self-transcendence stands in contrast to self-referential mental processing, and meditation practice is generally designed to lead the practitioner from self-referential to self-transcendent mental states.
Mind wandering and the default mode network. Despite these psychological and physiological benefits, less than 15 percent of the American population meditates.31 There are many barriers to maintaining a regular practice. Among them are the esoteric theological terms used by schools of meditation, the association of meditation with Eastern spiritual traditions, the challenge of assessing the reliability of teachers in the absence of a formal accreditation structure, the difficulty of stilling the mind, time constraints, and the many distractions of everyday life. When novice meditators first sit still and close their eyes, they are rarely able to focus their attention away from the stream of self-referential thoughts that typically fill the mind. Meditation researchers refer to this as “mind-wandering,” and it distracts novice meditators from entering the elevated emotional states of self-transcendence reported by experienced meditators.32 Mind-wandering occupies about half of our waking life and is associated with a decrease in happiness.33
Mind-wandering correlates with increased neural activity in the default mode network (DMN), the primary network of brain regions active in self-referential processing.33–37 Activation of the DMN is associated with mental explorations referenced to oneself, including thinking about the future.38 In addition, the DMN’s self-referential mental and neurological activity is the antithesis of the self-transcendent altered states of consciousness described by meditation adepts,39 defined by Goleman and Davidson32 as those with 10,000 hours of practice or more. A primary purpose of traditional meditation training is to gradually reduce the unhappiness and self-absorption of self-referential mental activity and increase the phenomenological experience of self-transcendent states.
The primary poles of the DMN are in the centerline of the brain, coordinated by the midprefrontal cortex in the anterior regions and the posterior cingulate cortex and adjacent precuneus in the posterior regions. The DMN activates during internal-oriented tasks or external stimulus-independent thoughts and deactivates whenever any external-oriented task network activates (also called task-positive networks [TPNs]). The DMN is named the default network because it is the default state to which the brain returns whenever TPNs downregulate as the brain disengages from external-oriented tasks. The DMN has a rich neural network connecting it with other brain regions. Increased DMN activity has been linked to impairments in executive functions, such as memory, attention, flexibility, inhibition, planning, and problem-solving.40,41
Neuroplastic remodeling in meditation. The hippocampus, a key region for encoding and retrieving memories, has been shown to be dramatically affected by meditation practice. These effects are evident in various dimensions of hippocampal function. First, functional neuroimaging studies have consistently shown that the hippocampus is engaged during meditation experiences (i.e., more strongly activated and connected).42–46 Moreover, continued meditation practice has also been associated with increases in hippocampal gray matter density and volumes,47–51 as well as enhanced structural (i.e., higher fiber integrity) connections.52 Positive correlations with medial temporal lobe gray matter density and increased levels of mindfulness indicate that this link is functionally relevant.53 This is further corroborated by studies providing evidence for the positive effect of meditation on working memory capacity and increased specificity of autographical memory.19,54–56
Meditation is a general term that includes many variants. Church39 organized these variants into seven categories based on their primary focuses. The first includes practices that focus on the breath. The second emphasizes observing one’s thoughts. The third has the practitioner evoke feelings of loving-kindness and compassion. The fourth category uses movement and includes qigong, Sufi dancing, tai chi, and Buddhist walking meditation; other meditative styles that include physical awareness include yoga nidra, body scanning, and progressive muscle relaxation. The fifth category of meditation uses verbal, vocal, or other auditory cues, such as chanting, prayer, gongs, hymns, saying the rosary, or repeating a mantra. The sixth employs visualization; visualizers might picture a sacred image, such as a Tibetan yantra tapestry, the crucifix, or the face of a saint. The final style has as its starting point the contemplation of an inspirational writing or person; inhabiting or imitating a meditation adept’s mindset can provide a template for the contemplator’s attainment of a self-transcendent state. All seven of these practices have, as one goal, the suppression of mind-wandering and self-referencing. Magnetic resonance imaging (MRI) studies show that experienced meditators are able to downregulate the activity of the DMN and thereby acquire self-transcendent “unitary consciousness.”32
EcoMeditation as a combination of evidence-based practices. EcoMeditation is a novel form of meditation designed to overcome the most common barriers to practice. Rather than instructing the practitioner to attempt to stop the mind-wandering and self-referential thinking of the DMN, it provides a sequence of active physical tasks that keep the TPN active (e.g., “Slow your breathing to six seconds per inbreath” and “Relax your tongue on the floor of your mouth.”). It does not rely on any philosophical, spiritual, religious, or cognitive framework. The instructions for EcoMeditation comprise seven simple steps designed to produce relaxed alertness (EcoMeditation.com).57 This makes its practice relatively easy for both inexperienced and experienced meditation practitioners.
EcoMeditation combines commonly used stress-reduction skills, such as mindfulness, heart coherence, emotional freedom techniques (EFT), and neurofeedback. It draws on elements of four empirically established techniques: the quick coherence technique for regulating heart rate variability,58 EFT,59 mindfulness meditation,60 and neurofeedback.60,61 EcoMeditation is therefore not aligned with a particular spiritual philosophy or orientation and does not require prior training or practice. The seven steps include 1) imagining the breath flowing in and out through the center of the chest; 2) slowing the breath to six seconds per inbreath and six seconds per outbreath; 3) acupressure on acupoints associated with relaxation; 4) relaxing the tongue on the floor of the mouth; 5) noticing the volume of space inside the body, especially between the eyes; 6) recalling a figure with positive emotional associations, such a mentor or archetype; and 7) contemplating positive affirmations.
An electroencephalogram (EEG) study found that the seven physiological cues used in EcoMeditation produced the brain wave patterns characteristic of advanced meditators, even in novices during their first attempt.62 Another study examined changes in psychological and physiological markers in 34 participants following a two-day EcoMeditation workshop.23 Improvements were found in psychological symptoms of anxiety, depression, and pain, as well as physiological measures, including cortisol and resting heart rate. Happiness levels also increased significantly. Similar results were found in a group of 208 participants practicing EcoMeditation at a daylong group workshop.39 The instructions for EcoMeditation are designed to keep the brain’s TPN at least minimally engaged; this engagement is hypothesized to be sufficient to prevent activation of the DMN in novices.62
Meditation produces mental states of calmness and focus when successfully practiced. When the neural pathways associated with these states are activated repeatedly, neuroplasticity is triggered. Over time, this produces structural changes in the brain. The time frames required can be surprisingly short. In as little as eight weeks, practicing for 12 minutes a day can produce measurable brain changes.41 For example, meditation adepts exhibit marked changes in brain anatomy. The volume of stress-processing structures, such as the amygdala, shrink, while learning centers, such as the hippocampus, grow.32 In time, neuroplasticity turns the transient self-transcendent states experienced by novices into the durable personality traits of meditation adepts.
When comparing the extent of neuroplastic changes to the volume of brain regions, three meditative practices result from activation of brain regions. These are meditating in groups, extending a sense of compassion toward others, and increasing the intensity of the experience.32–39 EcoMeditation includes instructions intended to activate these triggers. The meditator is instructed to imagine extending compassion first to another person, then generally outward to the whole universe. Further instructions have the meditator increase the intensity of the experience. Finally, EcoMeditation is frequently practiced in groups, including virtual groups assembled via video conferencing or applications (apps). The most widely used app, Insight Timer, provides a real-time count of those using the app in a virtual group; in 2020 its community of 18 million meditated for 5.6 billion minutes.63
The insula and prosocial emotions. Compassion is associated with the activation of brain regions that govern prosocial behavior, especially the insula.32,64 A meta-analysis of 21 neuroimaging trials found the insula to be one of the brain regions that increases in size in meditators.20 The insula is a region of tissue located deep inside the crevice separating the brain’s temporal lobe from the frontal and parietal lobes. It plays a role in various functions, including socioemotional processing and interoception, or the sense of the internal state of the body. The insula serves an important role in the subjective feeling component of emotions.
The insula contains a large concentration of Von Economo neurons. These neurons facilitate the integration of information from many different parts of the brain. These specialized cells are found in only a few species of animals that form highly organized social groups, including humans, apes, monkeys, whales, and elephants.65 A meta-analysis of 78 functional MRI (fMRI) studies found the insula to be one of the brain regions consistently upregulated across meditation methods.5
The insula is part of the “caretaking circuit” found in mammals who nurture their young. In humans, it is also activated in prosocial tasks related to family, tribe, and members of our social networks. It is associated with the emotions that connect us to other human beings. These social emotions include pride, disgust, guilt, gratitude, resentment, embarrassment, contempt, and lust.32 Thus, in social settings, Von Economo neurons in the insula help us recognize emotions, such as disgust, approval, and guilt, in other people’s facial expressions. They enable humans to enjoy jokes, take offense when ignored by an acquaintance, or feel gratitude when hugged by a friend.
Activation of the insula is also associated with subjective feelings of happiness, kindness, and empathy.32 People who are more sensitive to emotional cues from others have greater insula activation and score higher on tests of empathy than others.41 The insula is active during meditation sessions, especially when the meditator is deliberately invoking feelings of kindness and compassion toward others. MRI scans show that experienced meditators can produce over five times the activation of the insula and other structures in the brain’s “empathy circuits” as nonmeditators.32
Finally, as mentioned earlier, meditation has a profound effect on autobiographical memory, enabling enhanced retrieval of specific life episodes.55 These effects are thought to be mediated by increasing activity and even structural growth in the hippocampus, the core human memory structure.51
In the current study, we sought to test the impact of a secular, physiological method of meditation. We hypothesized that EcoMeditation would produce increases in neural communication in brain regions associated with compassion, prosociality, and autobiographical memory, and decreases in self-referencing networks, such as the DMN, and that these changes would be found in the experimental, but not the control, group.
Methods
Participants. In total, 56 adults responded to a call to participate in the study. Social media sites (e.g., Facebook, LinkedIn) were used to advertise the study and list inclusion and exclusion criteria. The study was open to both experienced meditators and novices or inexperienced meditators over 18 years of age. Exclusion criteria included a known previous or current mental health diagnosis (e.g., mood or anxiety disorder, personality disorder, psychotic disorder, posttraumatic stress disorder [PTSD], or substance use disorder), prior head trauma, current recreational drug usage, and current use of any prescription medication that affects the central nervous system (CNS).
Both meditators and nonmeditators were eligible to participate. Experienced meditators were classified as those participants who self-reported a meditation frequency and duration of practice of at least twice a week for 30 minutes or more for a year or more. Of the 56 individuals who responded, 32 were classified as experienced meditators and 24 as inexperienced. An online randomization tool was used to allocate the participants to either the experimental or control group. After accounting for withdrawals in the study, computer-generated random allocation resulted in 17 participants allocated to the EcoMeditation group (11 inexperienced and 6 experienced meditators) and 21 to the control intervention (13 inexperienced and 8 experienced meditators). Of this sample, 33 participants attended the preimaging fMRI scan (5 did not begin the trial) and 25 completed the postimaging scan. Therefore, the final sample consisted of 25 participants (18 female, 7 male) aged 24 to 61 years (mean: 41.86; standard deviation [SD]: 11.37); however, one participant did not complete the final postimaging survey. Fifteen participants were in the EcoMeditation arm and 10 in the control intervention. Of the total sample, 75 percent were married or lived with another person, 70 percent held a bachelor’s degree or higher, 37.5 percent worked in education, 20.8 percent worked in healthcare, and 20.8 percent were students. The trial was registered with the Australian New Zealand Clinical Trials Registry (Trial ID: ACTRN12619001555145) and ethical approval was provided by the University Human Research Ethics Committee. Enrollment and data collection were conducted from October to December 2019. All participants signed informed consent prior to engaging in the trial.
Psychological measures. Demographic information was collected prior to the first fMRI scan and included information about length and frequency of prior meditation practice and estimated total lifetime hours (TLH) of meditation. A battery of measures was also administered via an online survey instrument. These included five assessments.
Patient Health Questionnaire (PHQ). The PHQ66 is a validated diagnostic tool for mental health disorders, containing mood (PHQ-9), anxiety, alcohol, eating, and somatoform modules, as covered in the longer, original instrument (Primary Care Evaluation of Mental Disorders [PRIME-MD]). The internal consistency and construct validity of each subscale of the full PHQ has been determined in previous studies.66 Reviews have demonstrated that the full PHQ is highly sensitive to change in monitoring treatment outcomes.67
30-item Revised Mystical Experiences Questionnaire (MEQ30). The MEQ3068 is designed to evaluate whether a participant has had a mystical experience, defined as “the experience of profound unity with all that exists, a felt sense of sacredness, a sense of the experience of truth and reality at a fundamental level (noetic quality), deeply felt positive mood, transcendence of time and space, and difficulty explaining the experience in words.” The MEQ30 contains 30 descriptive statements divided into four categories: mystical, positive mood, transcendence of time and space, and ineffability. Each item is rated on a six-point scale, where 0 equals “none or not at all”; 1 equals “so slight I cannot decide”; 2 equals “slight”; 3 equals “moderate”; 4 equals “strong (equivalent in degree to any previous strong experience or expectation of this description)”; and 5 equals “extreme (more than ever before in my life and stronger than 4).” The MEQ30 was shown to be both reliable and valid and has been the standard for measuring mystical experiences for decades.68 Because contemplative practices, such as meditation, can induce these altered states that can have powerful effects on the individual, we sought to measure the impact of EcoMeditation on these experiences.
Brief PTSD Checklist (Brief PCL). A two-item screening tool for PTSD was included.69 It is an abbreviated form of the PCL and has been assessed as having psychometric properties comparable to the full instrument.69
Pain and Happiness. General happiness was rated using the Happiness Scale,70 a 10-point Likert scale to indicate if respondents felt happy in general, from 0 (not at all) to 10 (very). The Numeric Pain Rating Scale71 is based on a self-rated average of pain experienced in the previous 24 hours, ranging from 0 (not at all) to 10 (worst pain imaginable).
Procedure. The online questionnaire was created using PsychData, a secure online system for psychological research. After recruitment and prior to commencement of data gathering, a detailed explanatory statement with informed consent was provided to participants. Demographic information was then collected, as well as the self-report measures. The data was then transferred to the IBM Statistical Package for the Social Sciences (SPSS) version 26.0 for statistical analysis. The fMRI scan was conducted at a local diagnostic imaging center. Immediately afterward, participants were provided with an audio track and instructed to listen to it once per day for the four-week trial. A short message service was used twice per week to remind all participants to continue the intervention. At the end of the four weeks, participants were again scanned and completed their postintervention survey through an online link.
The experimental group listened to a 22-minute audio EcoMeditation track. The first five minutes led them through each of the seven relaxation steps. The middle section repeated various steps and was intended to provide just enough mental stimulation to keep their attention and keep the TPN engaged. The final two minutes oriented them back to everyday reality. To control for as many variables as possible, the 22-minute audio provided to the control group was designed to be as similar as possible to the EcoMeditation track. The same background music and narrative voice was used. Participants in the control group were instructed to relax and think about a recent vacation while breathing mindfully. These three interventions—relaxation, visualization, and mindful breathing—were designed to provide a plausible active control. The primary omission in the control track was the instructions for the seven physiological cues used in EcoMeditation.
MRI acquisition. All images were acquired using a 3.0-Simens Skyra scanner. A resting-state echo-planar imaging scan (36 axial slices; 3 × 3mm in-plane resolution; slice thickness, 3.0mm; 280 volumes; TR/TE, 2210/30ms) was acquired for each participant. Participants were instructed to rest with their eyes open. A high-resolution T1-weighted fast field echo structural scan (92 slices; 1.0mm isovoxel resolution; TR/TE, 2400/2.26ms) was also acquired. All participants had an initial (preintervention) brain scanning session and a second (postintervention) scan four weeks later. All scans were completed between 8:00 a.m. and 4:00 p.m., after participants were presented with safety questions. The MRI scans were examined for intracranial structural abnormalities by the radiologist at the diagnostic center. There were two participants who required further investigation and were referred to their general practitioners, as required by the informed consent process.
fMRI is widely used to map brain activity. fMRI exploits the local increase in blood flow, and hence blood volume and blood oxygenation, that occurs to support the resulting increase in metabolic demand, instead of detecting neuronal activity directly. Most conventional fMRI studies are based on the blood oxygenation level-dependent (BOLD) effect, which describes the increase in fMRI signal due to the change in blood oxygenation and blood volume secondary to the increase in blood flow. Resting state fMRI (rsfMRI) is a technique that, in the absence of a specific task, assesses slow-wave synchronization in the fMRI signal to infer patterns of functional connectiveness between brain regions. Whereas task fMRI is geared toward detecting activation differences between groups or conditions, rsfMRI is aimed at detecting changes in the interaction of different brain regions (i.e., increases or decreases in communication between them).
rsfMRI processing. rsfMRI preprocessing was completed using MATLAB R2015b (MathWorks Inc.; Sherborn, US), Statistical Parametric Mapping software (SPM12, Wellcome Trust Centre for Neuroimaging; University College London, UK), and functional connectivity toolbox version 17 (CONN). CONN is a MATLAB-based cross-platform application for the computation, display, and analysis of fMRI data. The first three volumes of each run were discarded to avoid signal instability. Subsequently, images were motion corrected using rigid body linear transformation and unwarping, followed by slice-timing correction. Motion parameters were extracted and used as subject-level regressors. Next, the CONN algorithm for outlier detection was applied (i.e., ART-based identification of outlier scans). For most participants, no scans had to be removed, but for eight participants, between two and 24 out of 554 scans were removed, and this was accounted for by subject-level regressors. Subsequently, normalization to Montreal Neurological Institute (MNI) space was performed based on the standard SPM MNI-152 T1 template. Finally, the functional data was smoothed using an 8x8x8 FWHM Gaussian kernel.
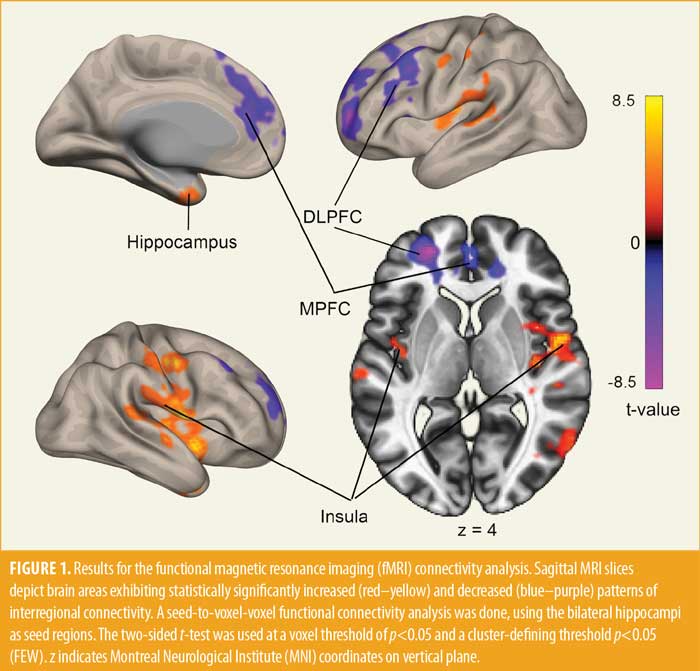
For the second level statistical analysis, we conducted a seed-to-voxel-voxel functional connectivity analysis, using anatomical seed-regions of interest definitions of the FSL Harvard-Oxford Atlas, as implemented by CONN. Guided by our prediction, we chose the bilateral hippocampi as our seed regions for the analysis; we tested for changes in connectivity originating in the left and right hippocampus. The type of intervention (EcoMeditation vs. control) was the main regressor of interest. In addition, further nuisance covariates were entered, including meditator status (inexperienced vs. expert), intervention compliance (days listened to the meditation), motion regressors (from the realignment procedure), and invalid images (from the ART procedure). The data was further band-pass filtered using the default values of 0.008 to 0.09Hz and corrected for noise components from cerebral white matter and cerebrospinal areas using the CompCor denoising algorithms implanted as a default in CONN.72 To detect changes due to EcoMeditation, we performed a two-sided comparison of pre- versus postintervention resting state connectivity for the EcoMeditation group. The two-sided test was used to detect increases and decreases in brain connectivity. A voxel threshold of p less than 0.05 and a cluster-defining threshold p less than 0.05 (FEW) was employed.
Results
Data were imported to SPSS Version 26 for analysis. Missing values analysis indicated that missing data were considered to be randomly missing (p=1.000) and not systematically tied to other variables. Accordingly, expectation maximization (EM) substitution was used to calculate values for missing data. Visual inspection of histograms and boxplots suggested that the data were approximately normally distributed. In total, 33 participants who were randomized from the original 56 attended the first fMRI scan. Limited appointment availability at the imaging facility was cited as the main reason the remainder did not attend. Twenty-five participants completed the final fMRI scan, of which 24 completed the postimaging survey. Due to the low numbers of experienced meditation practitioners in the sample, as well as their uneven distribution between groups, no analysis of the effect of meditation experience was possible. A Chi-squared constancy test indicated, however, that there was no significant imbalance in mediator types across the EcoMeditation and control conditions (χ2=0.529, p=0.467).
EcoMeditation participants reported practicing their meditation on average 21.62 days (2.5 days less than the control group) across the 28-day trial. However, this difference was not significant (p=1.185).
Psychological outcomes. Measured outcomes for pre- and posttest time points are displayed by intervention type in Table 1 (EcoMeditation) and Table 2 (control). In the EcoMeditation group, mean anxiety scores increased significantly (p=0.012), and this difference was large (d=0.75). Depression scores also increased significantly (p=0.006), with a medium effect size (d=0.65). Mystical experience scores increased significantly (p<0.001), and the effect was large for both the EcoMeditation (d=1.07) and control groups (d=2.05).
Pre- and posttest scores for each MEQ30 factor (mystical, positive mood, transcendence of time and space, and ineffability) are displayed in Table 3 (EcoMeditation) and Table 4 (control). In the EcoMeditation group, mean mystical experience factor scores significantly increased, and the effect was large for each factor: mystical (d=0.82), positive mood (d=0.81), transcendence of time and space (d=1.14), and ineffability (d=1.88). For the control group, mean mystical experience factors scores increased significantly (p=0.001), as did transcendence of time (p<0.001) and ineffability (p=0.002). However, positive mood did not significantly improve.


Six two-way mixed ANOVAs were then run to determine whether changes in anxiety (General Anxiety Disorder-7-item [GAD-7]), depression (PHQ-9), somatic symptoms (PHQ-15), mystical experiences (MEQ30), happiness, and pain were different for the two groups over time. Specifically, the ANOVAs tested whether there was an interaction between the type of intervention (between-subjects factor in experimental and control groups) and time (within-subjects factor), consisting of two time points (pre- and posttest for each group). Assumption testing revealed one outlier (case 24); however, the case was retained since examination of studentized residuals revealed no values exceeding ±3.0. Scores were approximately normally distributed as assessed by boxplots and normal Q-Q plots. There was homogeneity of variances, as assessed by Levene’s test of homogeneity of variance (p>0.05). There was homogeneity of covariances, as assessed by Box’s test of equality of covariance matrices (p>0.05).
There was no statistically significant interaction between group and time on anxiety (F[1, 22]=3.34, p=0.081, partial eta [η]2=0.132). The main effect for time showed a statistically nonsignificant difference in anxiety scores between time points (F[1, 22]=1.97, p=0.175, partial η2=0.082). The main effect for group showed a statistically nonsignificant difference in anxiety scores between intervention type (F[1, 22]=0.99, p=0.330, partial η2=0.043).
The interaction between group and time for depression symptom severity was statistically nonsignificant (F[1, 22]=1.02, p=0.323, partial η2=0.044). The main effect for time showed a statistically significant difference in depression scores at the different time points (F[1, 22]=10.76, p=0.003, partial η2=0.328). Posttest depression scores were 1.34 (95% confidence interval [CI]:0.49, 2.19), higher than pretest depression scores (p=0.003). The main effect for group showed no statistically significant difference in depression scores between intervention type (F[1, 22]=0.36, p=0.553, partial η2=0.016).
The interaction between group and time on somatic symptom severity was statistically nonsignificant (F[1, 22]= 0.00, p=0.994, partial η2=0.000). The main effect for time showed a statistically nonsignificant difference in somatic symptom scores between time points (F[1, 22]=3.45, p=0.077, partial η2=0.136). The main effect for group showed no statistically significant difference in somatic symptom scores (F[1, 22]=1.14, p=0.297, partial η2=0.049).
The interaction between group and time was not statistically significant for mystical experience scores (F[1, 22]=0.75, p=0.395, partial η2=0.033). The main effect for time showed a statistically significant difference in mystical experiences at the different time points (F[1, 22]=41.84, p<0.001, partial η2=0.655). Posttest mystical experience scores were 45.16 (95% CI: 23.23, 45.16), higher than pretest MEQ30 scores (p<0.001). The main effect for group indicated there was no statistically difference in mystical experience between intervention type (F[1, 22]=1.76, p=0.198, partial η2=0.074).
There was no statistically significant interaction between group and time on happiness (F[1, 22]=0.00, p=0.953, partial η2=0.000). The main effect for time showed a statistically nonsignificant difference in happiness scores between time points (F[1, 22]= 0.69, p=0.414, partial η2=0.031). The main effect for group showed there was a statistically nonsignificant difference in happiness scores between intervention type (F[1, 22]=0.00, p=0.957 partial η2=0.000).
There was no statistically significant interaction between intervention type and time on pain (F[1, 22]=0.38, p=0.543, partial η2=0.017). The main effect for time showed a statistically nonsignificant difference in pain scores between time points (F[1, 22]=1.03, p=0.321, partial η2=0.045). The main effect for group showed a statistically nonsignificant difference in pain scores between intervention type (F[1, 22]=0.30, p=0.590, partial η2=0.013).
A nonsignificant main effect for time was obtained (F[1, 22]=2.17, p=0.155, partial η2=0.09), with posttest PTSD scores being nonsignificantly higher than pretest scores. A nonsignificant effect for intervention type was found (F[1, 22]=0.10, p=0.753, partial η2=0.01). There was no statistically significant interaction between time and intervention type (F[1, 22]=0.48, p=0.496, partial η2=0.02).
rsfMRI Outcomes. As shown in Figure 1 and Table 5, the EcoMeditation group showed significant increased connectivity between the bilateral hippocampus and bilateral insula, compared to preintervention. In addition, we observed significant decreases of connectivity between the bilateral hippocampus and the midprefrontal and left dorsolateral prefrontal cortices. In contrast, performing the same analysis in the control group did not reveal changes in connectivity patterns.
Discussion
This study was the first to examine the effects of EcoMeditation using MRI. It tested the method against an active control that included relaxation, visualization, and mindful breathing. The control intervention was designed to be as similar as possible to EcoMeditation, omitting only EcoMeditation’s seven specific physiological cues. This study built on an earlier pilot trial using EEG,62 which found that inexperienced meditators practicing EcoMeditation could quickly acquire the elevated brain states characteristic of long-term meditation adepts. This was also the first randomized, controlled trial (RCT) of EcoMeditation.
We observed patterns of functional connectivity between brain regions in those practicing EcoMeditation that were not present in the control group. As we predicted, one of the two primary modes of the DMN, the medial prefrontal cortex, was less connected after participants had completed a month of EcoMeditation. The second notable difference between the groups was increased activation of the insula, a region of the brain that processes social relationships and compassion, in the EcoMeditation group. EcoMeditation was associated with a shift in brain function away from networks involved in self-referencing and toward those implicated in self-transcendence. Though most of the participants were inexperienced meditators, the results reflected brain activity similar to that found in experienced meditators. This is consistent with the literature, demonstrating that when inexperienced meditators use effective techniques, “strong echoes of those brain patterns found in more experienced meditators” are observed.32,73
The rsfMRI analysis showed that the four weeks of EcoMeditation led to increased functional connectivity between the bilateral hippocampus and bilateral insula. In addition, we observed decreased functional connectivity between the bilateral hippocampus and the medial prefrontal and dorsolateral prefrontal cortices. The control group showed none of these changes in connectivity. The hippocampus is known for its function in the encoding, storage, and retrieval of declarative memories, both semantic as well as autobiographic. Previous studies have suggested that the connections between the insula and hippocampus mediate the encoding and retrieval of emotionally arousing information.74,75
The prefrontal cortex manages complex cognitive control processes, such as executive function, attention, planning, problem-solving, and emotional inhibition. There are many neuropsychological case histories showing that damage to the prefrontal cortex leads to emotional dysregulation, such as socially inappropriate crying and laughter. However, over-engagement of these emotional control processes can lead to inappropriate verbal bluntness and reduced emotional connection with others.76 After four weeks of EcoMeditation, we observed decreased functional influence of these prefrontal control processes on the hippocampal memory system.
The increase of hippocampal-insula connectivity, in concert with decreased prefrontal-hippocampal connectivity, suggests that EcoMeditation led to a decrease in emotional suppression, an increase in the encoding and retrieval of emotional information, and an enhanced capacity for compassion. The reduction of activity in the midprefrontal cortex, one of the two nodes of the DMN, is associated with reduced mind-wandering, less self-referential processing, greater self-transcendence, and increased happiness.32,41
It is notable that the results of this trial showed changes in brain function similar to those identified in expert meditators. Tibetan monks, for instance, attend three-year, three-month, and three-day retreats, meditating 10 to 14 hours per day. Some of the meditation adepts studied have attended three or more of these retreats over the course of 20 or 30 years of meditative practice and might have accumulated over 60,000 TLH, leading to extraordinary self-transcendent states, as measured by fMRI.32 This study showed that it is possible for inexperienced meditators to acquire similar brain states after only four weeks. For these individuals, EcoMeditation removes some of the barriers to practice, making meditation accessible to members of complex industrialized societies.
One point of difference between the patterns found in study participants and meditation adepts is that we did not observe significant changes in the posterior cingulate cortex and precuneus. These regions are in the back of the brain and are one of the two poles of the DMN, the other being the midprefrontal cortex, in which we did observe change. This region deactivates during attentionally demanding tasks and activates during the retrieval of episodic memories. We hypothesize that the moderate attentional focus required by the breath counting component of EcoMeditation engages the TPN just enough to counter deactivation of this node of the DMN. Further research is required to test this hypothesis.
Limitations. This study had several limitations. The sample size was moderate, which limits the potential to detect small differences between groups and increases the effect of outliers within groups. For instance, the scores for one participant in the EcoMeditation group were at the high end of moderate depression, with a PHQ-9 score of 14. Because of the small sample size, this skewed the results toward higher depression scores for that group. Further, the sample size was insufficient to run a comparison between the effects on experienced versus inexperienced meditators.
Missing data in the psychological questionnaires were also a limiting factor. There were six cases in the EcoMeditation group that did not supply all data (between 6.3% and 12.5%). In the control group, two cases were missing data (between 50.0% and 56.3%). EM was used to calculate missing values; however, this might have skewed the results. In addition, the adherence rate for EcoMeditation participants was lower than that of the control group. This might have been due to the increased psychological demand produced by EcoMeditation, compared to the simple control task of visualizing a recent vacation. A final limitation is that participants were not followed over time to determine whether the observed gains were durable.
The results we observed for emotional affect are puzzling and contradictory. MEQ30 scores for positive mood increased significantly in the EcoMeditation group; however, scores for depression and anxiety also increased significantly. How could one assessment find an increase in positive affect while the other found an increase in negative affect?
One possible explanation derives from studies showing that the insula is central to the sense of compassion.32 The instructions for EcoMeditation direct participants to connect emotionally with another person, as well as to the greater universe. Participants might have become more compassionate during the four weeks of the study, as evidenced by upregulation of the insula. One of the most prolific meditation researchers of the past two decades describes these results from another MRI study: “The more deeply immersed in the compassion meditation a person reported being, the stronger was this empathetic pattern—compassion seems to amplify empathy toward suffering.”32 This empathy can also trigger an awareness of the suffering of others, conceivably leading to an increase in depression and anxiety. Compassion for oneself and the suffering of others in the world might also lead to more sensitivity to that suffering, and hence greater negative affect.
The three other extant studies of EcoMeditation have found an increase in happiness and a decrease in anxiety and depression.23,39,62 Participants maintained these gains over time, with some samples showing a greater long-term effect than that observed in posttest scores.39 It would have been insightful to perform a follow-up assessment of the participants in this study, to determine whether the effects for mood were durable. The affect and durability questions will be elucidated by further research.
Conclusion
Clinical implications. This study has a number of clinical implications. Several psychopathologies have been linked to regions of the DMN. Downregulation of the DMN, as measured in this study, can reduce the risk of such diagnoses. Furthermore, in healthy populations, activation of the DMN is associated with stress and unhappiness. Regulation of the midprefrontal cortex, as measured in this study, can reduce stressful self-referential brain activity and promote a self-transcendent perspective. Because it is a physiologically based method that does not require participants to perform difficult mental feats, such as stilling the mind, EcoMeditation might produce a higher level of participant compliance than other forms of meditation, which are notoriously difficult to practice consistently.29,31
Phenomenological accounts supplied by participants in EcoMeditation studies emphasize that most participants found the method easy and accessible from their first attempt. The method does not require belief in a particular worldview or theological perspective and is devoid of the ideology of traditional schools of meditation. It is based on simple physiological cues, rather than complex and demanding mental instructions. Inexperienced meditators can quickly experience self-transcendent states, which provides a rewarding initial experience. These characteristics remove the primary barriers to entry for inexperienced meditators. EcoMeditation might therefore reinforce the development of a consistent practice, making the extensive health and psychological benefits of meditation accessible to a larger population.
Availability of Data and Materials
The datasets for this study can be found at this link: https://osf.io/cg6h9/?view_only=211012fbc4f24b78a04a47ff1ff73cb7
Author Contributions
PS coordinated the trial, collected the data, advised and contributed to manuscript preparation, and edited the final version. OB monitored data collection, analyzed the fMRI data, advised on manuscript preparation, and edited the final version. DC advised on the technique being investigated and supplied meditation for use, prepared the manuscript, and edited the final version. DS assisted with data analyses, and prepared and drafted the manuscript.
Acknowledgements
The authors acknowledge Queensland Diagnostic Imaging, Gold Coast, for their support with this trial.
References
- Black D, Slavich GM. Mindfulness meditation and the immune system: a systematic review of randomized controlled trials. Ann N Y Acad Sci. 2016;1373(1):13–24.
- Boccia M, Piccardi L, Guariglia P. The meditative mind: a comprehensive meta-analysis of MRI studies. Biomed Res Int. 2015;2015.
- Crenshaw CE, Crenshaw CB, Jr. EFT for Meditation. Energy Psychology Press; 2015.
- Dahl CJ, Lutz A, Davidson RJ. Reconstructing and deconstructing the self: cognitive mechanisms in meditation practice. Trends Cogn Sci. 2015;19(9):515–523.
- Fox KC, Dixon ML, Nijeboer S, et al. Functional neuroanatomy of meditation: a review and meta-analysis of 78 functional neuroimaging investigations. Neurosci Biobehav Rev. 2016;65:208–228.
- Saatcioglu F. Regulation of gene expression by yoga, meditation and related practices: a review of recent studies. Asian J Psychiatr. 2013;6(1):74–77.
- Sanada K, Montero-Marin J, Díez MA, et al. Effects of mindfulness-based interventions on salivary cortisol in healthy adults: a meta-analytical review. Front Physiol. 2016;7:471.
- Shapiro SL, Carlson LE. Mindfulness and self-care for the clinician. In: SL Shapiro, LE Carlson. The Art and Science of Mindfulness: Integrating Mindfulness into Psychology and the Helping Professions. American Psychological Association; 2017:115–126.
- Bowen S, Witkiewitz K, Clifasefi SL, et al. Relative efficacy of mindfulness-based relapse prevention, standard relapse prevention, and treatment as usual for substance use disorders: a randomized clinical trial. JAMA Psychiatry. 2014;71(5):547–556.
- Brewer JA, Elwafi HM, Davis JH. Craving to quit: psychological models and neurobiological mechanisms of mindfulness training as treatment for addictions. Psychol Addict Behav. 2013;27(2):366–379.
- Garland EL, Howard MO. Mindfulness-oriented recovery enhancement reduces pain attentional bias in chronic pain patients. Psychother Psychosom. 2013;82(5):311–318.
- Garland EL, Manusov EG, Froeliger B, et al. Mindfulness-oriented recovery enhancement for chronic pain and prescription opioid misuse: results from an early-stage randomized controlled trial. J Consult Clin Psychol. 2014;82(3):448.
- Kabat-Zinn J, Lipworth L, Burney R, Sellers W. Four-year follow-up of a meditation-based program for the self-regulation of chronic pain: treatment outcomes and compliance. Clin J Pain. 1987;3(1):60.
- Teixeira ME. Meditation as an intervention for chronic pain: an integrative review. Holist Nurs Pract. 2008;22(4):225–234.
- Goyal M, Singh S, Sibinga EM, et al. Meditation programs for psychological stress and well-being: a systematic review and meta-analysis. JAMA Intern Med. 2014; 174(3):357–368.
- Segal ZV, Teasdale JD, Williams JMG. Mindfulness-based cognitive therapy: theoretical rationale and empirical status. In Hayes SC, Follette VM, Linehan MM, eds. Mindfulness and Acceptance: Expanding the Cognitive-Behavioral Tradition. Guilford Press; 2004:45–65.
- Khoury B, Lecomte T, Fortin G, et al. Mindfulness-based therapy: a comprehensive meta-analysis. Clin Psychol Rev. 2013;33(6):763–771.
- Kuyken W, Warren FC, Taylor RS, et al. Efficacy of mindfulness-based cognitive therapy in prevention of depressive relapse: an individual patient data meta-analysis from randomized trials. JAMA Psychiatry. 2016;73(6):565–574.
- Chiesa A, Calati R, Serretti A. Does mindfulness training improve cognitive abilities? A systematic review of neuropsychological findings. Clin Psychol Rev. 2011;31(3):449–464.
- Fox KC, Nijeboer S, Dixon ML, et al. Is meditation associated with altered brain structure? A systematic review and meta-analysis of morphometric neuroimaging in meditation practitioners. Neurosci Biobehav Rev. 2014;43:48–73.
- Tang Y-Y, Hölzel BK, Posner MI. The neuroscience of mindfulness meditation. Nat Rev Neurosci. 2015;16(4):213–225.
- Deng W, Cheung S, Tsao S, et al. Telomerase activity and its association with psychological stress, mental disorders, lifestyle factors and interventions: a systematic review. Psychoneuroendocrinology. 2016;64:150–163.
- Groesbeck G, Bach D, Stapleton P, et al. The interrelated physiological and psychological effects of EcoMeditation. J Evid Based Integr Med. 2018;23:2515690X1875962.
- Zeidan F, Vago DR. Mindfulness meditation-based pain relief: a mechanistic account. Ann N Y Acad Sci. 2016;1373(1):114–127.
- Church D. Mind to Matter: The Astonishing Science of How Your Brain Creates Material Reality. Hay House Inc.; 2018.
- Fischer R. A cartography of the ecstatic and meditative states. Science. 1971;174(4012):897–904.
- Levin J, Steele L. The transcendent experience: conceptual, theoretical, and epidemiologic perspectives. Explore (NY). 2005;1(2):89–101.
- Murphy M. The Future of the Body: Explorations into the Further Evolution of Human Nature. Jeremy P. Tarcher, Inc.; 1992.
- Vieten C, Wahbeh H, Cahn BR, et al. Future directions in meditation research: recommendations for expanding the field of contemplative science. PLoS One. 2018;13(11):e0205740.
- Vago DR, Silbersweig DA. Self-awareness, self-regulation, and self-transcendence (S-ART): a framework for understanding the neurobiological mechanisms of mindfulness. Front Hum Neurosci. 2012;6:296.
- Clarke TC, Barnes PM, Black LI, et al. Use of yoga, meditation, and chiropractors among US adults aged 18 and older. NCHS Data Brief. 2018;325:1–8.
- Goleman D, Davidson RJ. Altered Traits: Science Reveals How Meditation Changes Your Mind, Brain, and Body. Avery; 2018.
- Killingsworth MA, Gilbert DT. A wandering mind is an unhappy mind. Science. 2010;330(6006):932.
- Christoff K, Gordon AM, Smallwood J, et al. Experience sampling during fMRI reveals default network and executive system contributions to mind wandering. Proc Natl Acad Sci U S A. 2009;106(21):8719–8724.
- Mason MF, Norton MI, Van Horn JD, et al. Wandering minds: The default network and stimulus-independent thought. Science. 2007;315(5810):393–395.
- Raichle ME, MacLeod AM, Snyder AZ, et al. A default mode of brain function. Proc Natl Acad Sci U S A. 2001;98(2):676–682.
- Simpson JR, Jr., Drevets WC, Snyder AZ, et al. Emotion-induced changes in human medial prefrontal cortex: II. During anticipatory anxiety. Proc Natl Acad Sci U S A. 2001;98(2):688–693.
- Buckner RL, Andrews-Hanna JR, Schacter DL. The brain’s default network: anatomy, function, and relevance to disease. In: Kingstone A, Miller MB, eds. The Year in Cognitive Neuroscience 2008. Blackwell Publishing; 2008:1–38.
- Church D. Bliss Brain: The Neuroscience of Remodeling Your Brain for Creativity, Resilience and Joy. Hay House Inc.; 2020.
- Fox KC, Spreng RN, Ellamil M, et al. The wandering brain: meta-analysis of functional neuroimaging studies of mind-wandering and related spontaneous thought processes. Neuroimage. 2015;111:611–621.
- Newberg A, Waldman MR. How Enlightenment Changes Your Brain: The New Science of Transformation. Penguin; 2017.
- Lou HC, Nowak, M, Kjaer TW. The mental self. Prog Brain Res. 2005;150:197–204.
- Lazar SW, Bush G, Gollub RL, et al. Functional brain mapping of the relaxation response and meditation. Neuroreport. 2000;11(7):1581–1585.
- Holzel BK, Ott U, Hempel H, et al. Differential engagement of anterior cingulate and adjacent medial frontal cortex in adept meditators and non-meditators. Neurosci Lett. 2007;421(1):16–21.
- Engstrom M, Pihlsgard J, Lundberg P, Soderfeldt B. Functional magnetic resonance imaging of hippocampal activation during silent mantra meditation. J Altern Complement Med. 2010;16(12):1253–1258.
- Kalyani BG, Venkatasubramanian G, Arasappa R, et al. Neurohemodynamic correlates of ‘OM’ chanting: a pilot functional magnetic resonance imaging study. Int J Yoga. 2011;4(1):3–6.
- Holzel BK, Ott U, Gard T, et al. Investigation of mindfulness meditation practitioners with voxel-based morphometry. Soc Cogn Affect Neurosci. 2008;3(1):55–61.
- Leung MK, Chan CC, Yin J, et al. Increased gray matter volume in the right angular and posterior parahippocampal gyri in loving-kindness meditators. Soc Cogn Affect Neurosci. 2013;8(1):34–39.
- Luders E, Toga AW, Lepore N, Gaser C. The underlying anatomical correlates of long-term meditation: larger hippocampal and frontal volumes of gray matter. Neuroimage. 2009;45(3):672–678.
- Luders E, Thompson PM, Kurth F, et al. Global and regional alterations of hippocampal anatomy in long-term meditation practitioners. Hum Brain Mapp. 2013;34(12):3369–3375.
- Luders E, Kurth F, Toga AW, et al. Meditation effects within the hippocampal complex revealed by voxel-based morphometry and cytoarchitectonic probabilistic mapping. Front Psychol. 2013;4:398.
- Luders E, Clark K, Narr KL, Toga AW. Enhanced brain connectivity in long-term meditation practitioners. Neuroimage. 2011;57(4):1308–1316.
- Murakami H, Nakao T, Matsunaga M, et al. The structure of mindful brain. PLoS One. 2012;7(9):e46377.
- Williams JM, Teasdale JD, Segal ZV, Soulsby J. Mindfulness-based cognitive therapy reduces overgeneral autobiographical memory in formerly depressed patients. J Abnorm Psychol. 2000;109(1):150–155.
- Heeren A, Van BN, Philippot P. The effects of mindfulness on executive processes and autobiographical memory specificity. Behav Res.Ther. 2009;47(5):403–409.
- Kozhevnikov M, Louchakova O, Josipovic Z, Motes MA. The enhancement of visuospatial processing efficiency through Buddhist Deity meditation. Psychol Sci. 2009;20(5):645–653.
- Eco Mediation. ecomediation.com. Accessed 24 Aug 2022.
- McCraty R, Zayas M. Cardiac coherence, self-regulation, autonomic stability, and psychosocial well-being. Front Psychol. 2014;5:1090.
- Church D. Clinical EFT as an evidence-based practice for the treatment of psychological and physiological conditions. Psychology. 2013;4(8):645–654.
- Davidson R, Kabat-Zinn J, Schumacher J, et al. Alterations in brain and immune function produced by mindfulness meditation. Psychosom Med. 2003;65(4):564–570.
- Fehmi L, Robbins J. The Open-Focus Brain: Harnessing the Power of Attention to Heal Mind and Body. Trumpeter; 2008.
- Pennington J, Sabot D, Church D. EcoMeditation and EFT (emotional freedom techniques) produce elevated brainwave patterns and states of consciousness. Energy Psychol Theory Res Treat. 2019;11(1):10.9769/epj.2019.11.1.jp
- Businesswire. Meditators spent over 10,000 years on Insight Timer in 2020, 5x more than Calm. 22 Dec 2020. https://www.businesswire.com/news/home/20201222005383/en/Meditators-Spent-Over-10000-Years-on-Insight-Timer-in-2020-5x-More-Than-Calm. Accessed 7 Sep 2022.
- Lutz A, Greischar LL, Perlman DM, Davidson RJ. BOLD signal in insula is differentially related to cardiac function during compassion meditation in experts vs. novices. Neuroimage. 2009;47(3):1038–1046.
- Namkung H, Kim SH, Sawa A. The insula: an underestimated brain area in clinical neuroscience, psychiatry, and neurology. Trends Neurosci. 2017;40(4):200–207.
- Spitzer RL, Kroenke K, Williams JB. Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study. Primary care evaluation of mental disorders. Patient health questionnaire. JAMA.1999;282(18):1737–1744.
- Kroenke K, Spitzer RL, Williams JBW, Lowe B. The patient health questionnaire somatic, anxiety, and depressive symptom scales: a systematic review. Gen Hosp Psychiatry. 2010;32(4):345–359.
- Barrett F, Johnson MW, Griffiths RR. Validation of the revised Mystical Experience Questionnaire in experimental sessions with psilocybin. J Psychopharmacol. 2015;29(11):1182–1190.
- Lang AJ, Stein MB. An abbreviated PTSD checklist for use as a screening instrument in primary care. Behav Res Ther. 2005;43(5):585–594.
- Abdel-Khalek AM. Measuring happiness with a single-item scale. Soc Behav Pers. 2006;34(2):139–150.
- McCaffery M, Beebe A. Pain: Clinical Manual for Nursing Practice. Mosby Elsevier Health Science; 1989.
- Behzadi Y, Restom K, Liau J, Liu TT. A component based noise correction method (CompCor) for BOLD and perfusion based fMRI. NeuroImage. 2007;37(1):90–101.
- Weng HY, Fox AS, Shackman AJ, et al. Compassion training alters altruism and neural responses to suffering. Psychol Sci. 2013;24(7):1171–1180.
- Critchley HD, Mathias CJ, Dolan RJ. Fear conditioning in humans: the influence of awareness and autonomic arousal on functional neuroanatomy. Neuron. 2002;33(4):653–663.
- Jin J, Maren S. Prefrontal-hippocampal interactions in memory and emotion. Front Syst Neurosci. 2015; 9:170.
- Butler E, Egloff B, Wilhelm F, et al. The social consequences of expressive suppression. Emotion. 2003;3(1):48–67.