
 by Takahiko Nagamine, MD, PhD
by Takahiko Nagamine, MD, PhD
Dr. Nagamine is with the Sunlight Brain Research Center in Hofu, Yamaguchi, Japan.
FUNDING: No funding was provided for this study.
DISCLOSURES: The author has no conflicts of interest relevant to the content of this article.
ABSTRACT: Objective. There are several conditions of treatable dementia. Among these, hyponatremia can cause transitory modification of cognitive functions.
Design. We treated a patient with cognitive decline after minor head injury who developed severe hyponatremia due to central salt wasting syndrome (CSWS).
Results. Head injuries can interfere with the normal neuroendocrine function of the hypothalamus and pituitary system, resulting in CSWS. A short-term infusion of isotonic saline solution might be useful in identifying CSWS.
Conclusion. Follow-up laboratory tests, including ones that test serum sodium leves, are recommended even in patients with minor head injury to diagnose potentially reversible conditions similar to dementia.
Keywords: Minor head injury, cognitive impairment, hyponatremia, central salt wasting syndrome (CSWS)
Innov Clin Neurosci. 2021;18(1–3):xx–xx
There are potentially reversible conditions similar to dementia. This patient group should be diagnosed early to start reversing the pathophysiology that could cause cognitive impairment. In this case study, we examined a patient with cognitive decline after minor head injury who developed severe hyponatremia.
Case Presentation
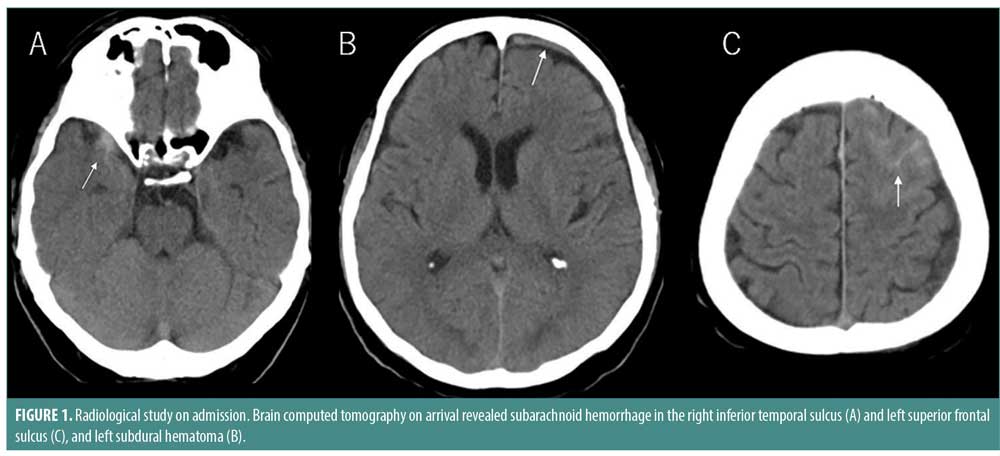
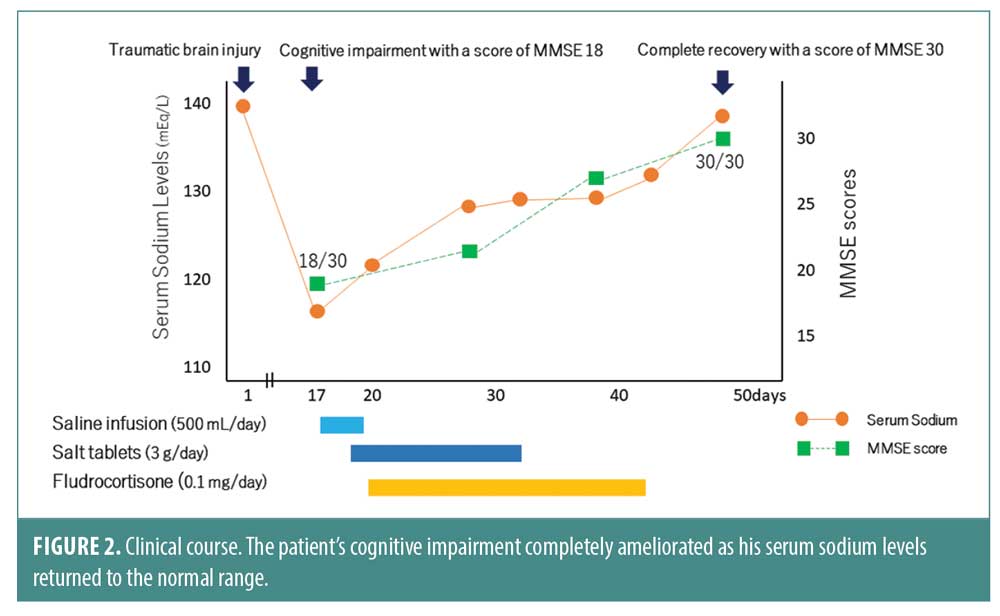
A 70-year-old male patient with no significant medical history was transferred to our hospital because of a traffic accident. On arrival, his consciousness was clear. Radiological examination revealed a small subarachnoid hemorrhage in the right inferior temporal sulcus and left superior frontal sulcus and small left subdural hemorrhage (Figure 1). He was admitted for surveillance following a diagnosis of minor head injury. After a week follow-up, he was discharged without neurological and cognitive problems. However, 10 days after being discharged, he showed short-term memory loss, difficulty concentrating, and mood changes, even though he was well enough to manage his activities of daily living. He was re-admitted to investigate the cause of cognitive impairment. He seemed to be well except for cognitive decline. Cognitive testing revealed a score of 18 out of 30 on the Mini-Mental State Examination (MMSE). Radiological examination at this time showed no abnormality. However, laboratory findings indicated severe hyponatremia of 117mEq/L with normal urine sodium level of 68mEq/L. His plasma osmolality was 239mOsm/kg/H2O, whereas urine osmolality was 424mOsm/kg/H2O. The serum antidiuretic hormone was high at 4.5pg/mL despite severe hyponatremia. A complete hormonal assessment was performed with serum cortisol, thyroid stimulating hormone (TSH), and serum free thyroxine (FT4) levels within the normal range, indicating normal adrenal and thyroid function. These findings match those of Syndrome of Inappropriate Secretion of Antidiuretic Hormone (SIADH). However, his serum sodium level remained low after one day strict water restriction of 800mL, and a short-term infusion of isotonic saline solution resulted in a slight increase in sodium level of 122mEq/L. Considering the possibility of central salt wasting syndrome (CSWS), sodium replenishment was performed with salt tablets of 3g/day and fludrocortisone of 0.1mg/day. After a month treatment of sodium replenishment, his serum sodium levels returned to normal of 138mEq/L and his cognitive impairment completely ameliorated with a score of 30 out of 30 on MMSE (Figure 2).
Discussion
There are several conditions of treatable dementia. Among these, hyponatremia can cause transitory modification of cognitive functions. A recent clinical study indicated that patients with hyponatremia had a 2.36-fold higher chances of suffering dementia.1 Moreover, patients with severe hyponatremia had higher risks of suffering dementia than patients with nonsevere hyponatremia, and a dose response relationship was observed between hyponatremia and dementia.1 The mechanism in which hyponatremia causes cognitive impairment is not completely understood. Recent research on hyponatremia using rats indicated that sustained reduction of serum sodium induced impaired long-term potentiation at hippocampal CA3-CA1 synapses due to the changes in glial glutamate uptake and glutamate metabolism.2
Head injuries interfere with the normal neuroendocrine function of the hypothalamus and pituitary system, thus, secreting antidiuretic hormone and/or natriuretic peptides and impairing sympathetic neural input to the juxtaglomerular apparatus. This leads to water reabsorption and an increase in sodium excretion, resulting in hyponatremia.3 The patients with serious head injury often showed severe hyponatremia owing to SIADH or CSWS. According to a recent prospective study on head injuries, hyponatremia correlated to the severity of brain damage as assessed by computed tomography, and the most common cause of it was SIADH.4 However, severe hyponatremia was reported not only in patients that had serious or minor head injuries.5 Clinicians should be aware of the possibility of severe hyponatremia that could cause cognitive impairment, even in minor head injury. Thus, follow-up laboratory tests including serum sodium level are recommended, even in patients with minor head injury.
Management of hyponatremia is challenging. The main problem of SIADH is excess fluid. Hyponatremia is dilutional in nature, while CSWS is characterized by extracellular fluid volume depletion caused by increased natriuresis. With SIADH, the treatment consists of free water restriction, while the treatment for CSWS is volume and salt replacement. It is critically important to distinguish CSWS from SIADH. Their treatments are opposite, but they have similar laboratory findings. A short-term infusion of isotonic saline solution may be useful in identifying CSWS, since the extracellular volume status of patients is a key point to differentiate these conditions.6
Conclusion
In conclusion, clinicians should include CSWS-induced hyponatremia among treatable dementias. CSWS is an unexpected electrolyte finding and a cause of cognitive impairment that can be found in patients with minor or serious brain injuries.
References
- Chung MC, Yu TM, Shu KH, et al. Hyponatremia and increased risk of dementia: a population-based retrospective cohort study. PLoS One. 2017;12(6):e0178977.
- Fujisawa H, Sugimura Y, Takagi H, et al. Chronic hyponatremia causes neurologic and psychologic impairments. J Am Soc Nephrol. 2016;27(3):766–780.
- Lieberman SA, Oberoi AL, Gilkison CR, et al. Prevalence of neuroendocrine dysfunction in patients recovering from traumatic brain injury. J Clin Endocrinol Metab. 2001;86(6):2752–2756.
- Lohani S, Devkota U. Hyponatremia in patients with traumatic brain inuury: etiology, incidence, and severity correlation. World Neurosurg. 2011;76(3–4):355–360.
- Csipak G, Hagau N. Cerebral salt wasting syndrome in patients with minor head trauma – two case reports. Rom J Anaesth Intensive Care. 2016;23(2):155–158.
- Cui H, He G, Yang S, et al. Inappropriate antidiuretic hormone secretion and cerebral salt-wasting syndromes in neurological Patients. Front Neurosci. 2019;13:1170.