

by Jonathan R. Scarff, MD
Dr. Scarff is a psychiatrist with the Behavioral Health Service Line at Kenner Army Health Clinic in Fort Lee, Virginia.
Funding: No funding was provided.
Disclosures: The authors have no conflicts of interest relevant to the content of this article.
Abstract: Postpartum depression (PPD) is often defined as an episode of major depressive disorder (MDD) occurring soon after the birth of a child. It is frequently reported in mothers but can also occur in fathers. There are no established criteria for PPD in men, although it could present over the course of a year, with symptoms of irritability restricted emotions, and depression. Risk factors include a history of depression in either parent, poverty, and hormonal changes. It might be associated with anxiety disorders and can adversely affect the father, family unit, and developing child. Treatment includes psychotherapy and pharmacotherapy. Clinicians are encouraged to screen for depression in men during the first year postpartum and to offer treatment or treatment referral if depression is present.
Keywords: Depression, postpartum, fathers, antidepressant, psychotherapy
Innov Clin Neurosci. 2019;16(5–6):11–14
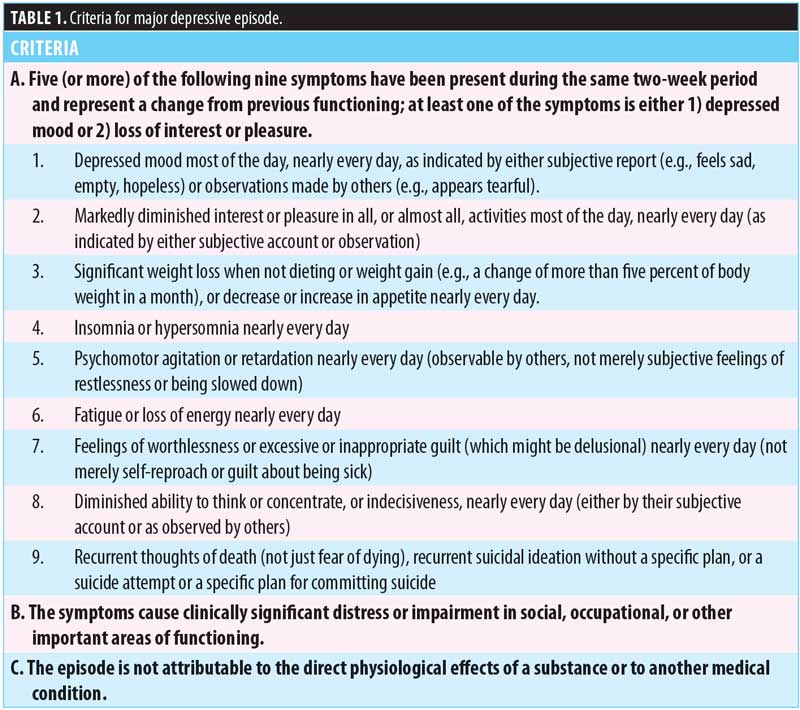
Numerous studies have examined the epidemiology, risk factors, treatment, and adverse effects of postpartum depression (PPD) in women; however, the condition is less understood in men. There is no universally accepted definition of PPD. The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) defines depression “with peripartum onset” as a major depressive episode (MDE) during pregnancy or within four weeks after parturition.1 Criteria for MDE are listed in Table 1. Although these criteria can be used to diagnose PPD in women and men, there might be subtle differences in onset and presentation between men and women. Occurring in approximately 8 to 10 percent of fathers, PPD has the highest prevalence within 3 to 6 months postpartum but might insidiously develop over a year rather than four weeks postpartum.2–4 Additionally, irritability, indecisiveness, and restricted range of emotion might be observed more frequently in men.5,6 This article discusses PPD in men with a focus on its prevalence, risk factors, adverse effects, diagnosis, and treatment.
Hypothetical Case
Mr. M was a 35 year-old attorney who presented to his primary care physician for “not sleeping.” Since the birth of his son four months previously, he reports sleeping only five hours and wakes earlier than desired, which resulted in low daytime energy. He reported a “frustrated” mood and no longer participated in activities he used to enjoy, such as exercising and watching sports with friends. He reported difficulty focusing on work assignments and admitted being more argumentative with family and coworkers. He reported increased appetite and weight gain over the previous two months. He reported feeling guilty that he was isolating himself from his family, and he questioned his worth and capabilities as a new father. He denied suicidal or homicidal ideation. Mr. M. reported depressed mood “off and on” since his early 20s but has not sought any treatment. Medical history was significant only for diet-controlled hyperlipidemia. Complete blood count, comprehensive metabolic profile, and thyroid function tests were within normal limits. Vital signs and physical examination revealed no abnormalities.
PPD Risk Factors
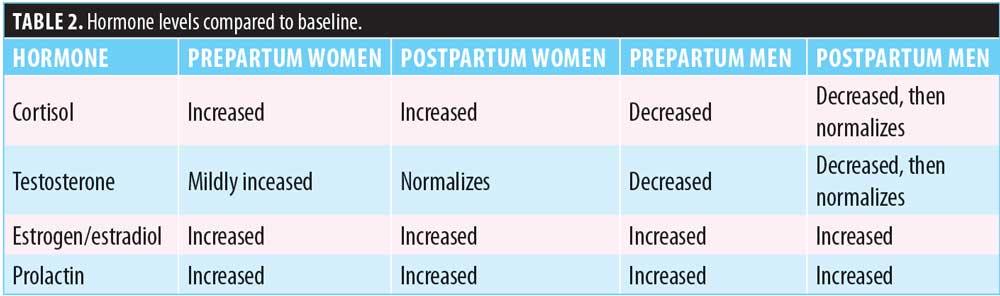
There are numerous potential risk factors that can contribute to the development of PPD in men, including history of depression, marital discord, poverty, maternal depression, and unintended pregnancy.5,7–9 Sleep deprivation and disrupted circadian rhythm, which have been positively correlated with depressive symptoms in women, might also increase a man’s risk of developing PPD.10 According to a review article by Kim and Swain,11 a father can experience hormonal changes during pregnancy and for several months following the birth of the child. Many of these hormonal changes are thought to assist in the formation of a strong father-child relationship. For example, Kim and Swain described studies linking decreased testosterone levels in new fathers to lower levels of aggression and increased sympathetic responses to a crying baby—effects that, in turn, are thought to strengthen the father’s attachment to the child. Kim and Swain also described studies linking increased estrogen levels in new fathers to more engaged paternal parenting behaviors. Additionally, increases in other hormones, such as cortisol, vasopressin, and prolactin, might be associated with more engaged paternal parenting and stronger parent-infant attachment.11 These hormonal changes, however, might predispose the father to experience PPD or exacerbate existing symptoms associated with PPD. For example, low testosterone has been directly linked to symptoms of depression in men,12 whereas low levels of estrogen, prolactin, vasopressin, and/or cortisol in new fathers might cause difficulties in father-infant bonding/attachment, which in turn can contribute to depressed mood in the father.11 Table 2 compares hormonal changes between men and women during prepartum and postpartum periods.11–13
PPD Comorbid Conditions
Comorbid postpartum anxiety might be comorbid with PPD; however, most studies of postpartum men included those who might or might not have had depressive symptoms. There are no studies examining the incidence or prevalence of comorbid PPD and anxiety disorders in men.
In a review of 43 multinational studies, up to 18 percent of postpartum men reported high levels of anxiety that did not meet criteria for a specific anxiety disorder.14 The incidence of generalized anxiety disorder (GAD) ranged from 3.4 to 4.3 percent, while up to five percent of men experienced symptoms of posttraumatic stress disorder (PTSD) several months postpartum.14 The incidence of panic disorder was approximately one percent in Australian men.15 Men might exhibit symptoms of or meet criteria for obsessive-compulsive disorder (OCD), such as excessive worry about the baby’s health, preoccupation with caretaking rituals, or intrusive thoughts of inadvertently harming the baby.16 However, one study found that although 3.4 percent of men met criteria for OCD in the third trimester, this decreased to 1.8 percent postpartum, matching the natural prevalence.17
PPD Adverse Effects
Preexisting depression in fathers has been shown to result in adverse effects for the father, family unit, and infant. One study found that infants of depressed fathers experienced higher levels of distress.18 A meta-analysis found that paternal depression adversely affected parenting behaviors and was associated with decreased sensitivity and increased hostility toward children.19 Children who live with a father with depression or other mental illness have a 33-to-70-percent increased risk of developing emotional or behavioral problems.20 Increases in paternal depression were associated with increased aggression in children from 0 to 4 years of age.21 Paternal depression was positively associated with delays in behavioral, emotional, and social development in 4 and 5-year-old children.22 Given the association between pre-existing paternal depression and adverse effects on the family, similar effects might be seen in fathers with PPD.
PPD Diagnosis
Despite no universally accepted diagnosis, PPD is often diagnosed through the clinical interview using DSM-5 criteria. Symptoms generally resemble those in women, with additional possible symptoms of indecisiveness, irritability, and emotional blunting that can present up to one year postpartum.2–6 Screening tools can be used to support the diagnosis. The Edinburgh Postnatal Depression Scale (EPDS) assesses postnatal depression and anxiety in men and women. Because men might be less expressive about their feelings and thus underreport symptoms, the scale uses a lower cutoff score for men.23 Even with this accommodation, its validity is limited by ambiguous items and limited detection of anxiety and depression symptoms in men.24 If the father cannot be directly assessed, the EPDS-Partner (EPDS-P) can be completed by the partner as a screening tool.25 Alternatively, the Patient Health Questionnaire (PHQ-9) demonstrated validity when screening for paternal PPD.26 Obtaining collateral information from family or friends, inquiring about increased irritability and somatic complaints, assessing for past depressive episodes, and comparing the father’s mental health status prior to, during, and after the pregnancy might further assist in diagnosis.
PPD Treatment
Because it is often understudied and undiagnosed, it is not surprising that there are no randomized, controlled trials (RCTs) evaluating treatment of PPD in men. However, because the symptoms constitute a MDE, which can present similarly among men and women, recommended treatments are the same for both sexes. Selective serotonin reuptake inhibitors (SSRI), such as sertraline, are recommended as first-line treatments, and they have been extensively studied.27–29 However, there is little evidence that antidepressants can prevent an episode of PPD, at least in women.30
Psychotherapy, such as cognitive behavior therapy (CBT) and interpersonal therapy (IPT), have been shown to be effective in alleviating depression, and these therapies were preferred by breastfeeding mothers.31,32 Furthermore, CBT demonstrated superiority to sertraline in a small RCT of mothers with PPD, with no reported benefit using combination treatment.33 Given the correlation between circadian rhythm disturbance and PPD, daily morning light therapy might reduce PPD symptoms, based on results from a small, open-label study of affected women.34 When a group of unaffected men was presented with a hypothetical scenario of PPD and treatment preferences, most preferred individual or couples psychotherapy to pharmacotherapy.35
Other interventions have been proposed to either prevent occurrence or ameliorate symptoms of PPD in men, such as support and acknowledgment of feelings and role conflicts.11 Educational programs incorporating both parents, either with or without PPD, might be beneficial.11,36 Support from employers, such as paid paternity leave, might also help fathers adapt to changes and stressors during the postpartum period.11
Conclusion
PPD has been associated with adverse consequences, yet it is a treatable condition. Clinicians are encouraged to screen for depression in fathers, particularly during the first year postpartum, especially if anxiety or risk factors are present. Antidepressant therapy or psychotherapy have been shown to be effective treatment modealities. Recognizing and treating paternal PPD can improve quality of life for the father and the family unit and decrease the risk for emotional and behavioral problems in children. Further studies should determine the prevalence, comorbidity, and efficacy of treatments for paternal PPD while including fathers from various demographic groups. Such groups could include single and two-father households, stepfathers, fathers from various socioeconomic, racial, and ethnic groups, and those residing in urban and rural areas.
Disclaimer
The views expressed in this article are those of the author and do not reflect official policy or position of the Department of Defense or the Department of the Army.
References
- American Psychiatric Association. Depressive Disorders. In: Diagnostic and Statistical Manual of Mental Disorders. Fifth Edition. Arlington, VA: American Psychiatric Association; 2013:153–188.
- Paulson JF, Bazemore SD. Prenatal and postpartum depression in fathers and its association with maternal depression: a meta-analysis. JAMA. 2010;303(19):1961–1969.
- Cameron EE, Sedov ID, Tomfohr-Madsen LM. Prevalence of paternal depression in pregnancy and the postpartum: An updated meta-analysis. J Affect Disord. 2016;206:189–203.
- Matthey S, Barnett B, Ungerer J, Waters B. Paternal and maternal depressed mood during the transition to parenthood. J Affect Disord. 2000;60(2):75–85.
- Berg AR, Ahmed AH. Paternal perinatal depression: making a case for routine screening. Nurse Pract. 2016;41(10):1–5.
- Madsen SA, Juhl T. Paternal depression in the postnatal period assessed with traditional and male depression scales. Int J Mens Health Gender. 2007;4:26–31.
- Fisher SD, Garfield C. Opportunities to detect and manage perinatal depression in men. Am Fam Physician. 2016;93(10):824–825.
- Rosenthal DG, Learned N, Liu YH, Weitzman M. Characteristics of fathers with depressive symptoms. Matern Child Health J. 2013;17(1):119–128.
- Nishimura A, Ohashi K. Risk factors of paternal depression in the early postnatal period in Japan. Nurs Health Sci. 2010;12(2):170–176.
- Gallaher KGH, Slyepchenko A, Frey BN, et al. The role of circadian rhythms in postpartum sleep and mood. Sleep Med Clin. 2018;13(3):359–374.
- Kim P, Swain JE. Sad dads: paternal postpartum depression. Psychiatry (Edgmont). 2007;4(2):35–47.
- Zarrouf FA, Artz S, Griffith J, et al. Testosterone and depression: systematic review and meta-analysis. J Psychiatr Pract. 2009;15(4):289–305.
- Berg SJ, Wynne-Edwards KE. Changes in testosterone, cortisol, and estradiol levels in men becoming fathers. Mayo Clin Proc. 2001;76(6):582–592.
- Leach LS, Poyser C, Cooklin AR, Giallo R. Prevalence and course of anxiety disorders (and symptom levels) in men across the perinatal period: a systematic review. J Affect Disord. 2016;190:675–686.
- Matthey S, Barnett B, Howie P, Kavanagh DJ. Diagnosing postpartum depression in mothers and fathers: whatever happened to anxiety? J Affect Disord. 2003;74(2):139–147.
- Leckman JF, Mayes LC, Feldman R, et al. Early parental preoccupations and behaviors and their possible relationship to the symptoms of obsessive-compulsive disorder. Acta Psychiatr Scand Suppl. 1999;396:1–26.
- Coelho FM, Silva RA, Quevedo Lde Á, et al. Obsessive-compulsive disorder in fathers during pregnancy and postpartum. Rev Bras Psiquiatr. 2014;36(3):271–273.
- Ramchandani PG, Psychogiou L, Vlachos H, et al. Paternal depression: an examination of its links with father, child and family functioning in the postnatal period. Depress Anxiety. 2011;28(6):471–477.
- Wilson S, Durbin CE. Effects of paternal depression on fathers’ parenting behaviors: a meta-analytic review. Clin Psychol Rev. 2010;30(2):167–180.
- Weitzman M, Rosenthal DG, Liu YH. Paternal depressive symptoms and child behavioral or emotional problems in the United States. Pediatrics. 2011;128(6):1126–1134.
- Narayanan MK, Naerde A. Associations between maternal and paternal depressive symptoms and early child behavior problems: testing a mutually adjusted prospective longitudinal model. J Affect Disord. 2016;196:181–189.
- Fletcher RJ, Feeman E, Garfield C, Vimpani G. The effects of early paternal depression on children’s development. Med J Aust. 2011;195(11-12):685–689.
- Matthey S, Barnett B, Kavanagh DJ, Howie P. Validation of the Edinburgh Postnatal Depression Scale for men, and comparison of item endorsement with their partners. J Affect Disord. 2001;64(2-3):175–184.
- Matthey S, Agostini F. Using the Edinburgh Postnatal Depression Scale for women and men-some cautionary thoughts. Arch Womens Ment Health. 2017;20(2):345–354.
- Fisher SD, Kopelman R, O’Hara MW. Partner report of paternal depres¬sion using the Edinburgh Postnatal Depression Scale-Partner. Arch Womens Ment Health. 2012;15(4):283–288.
- Santos IS, Tavares BF, Munhoz TN, et al. Patient Health Questionnaire-9 versus Edinburgh Postnatal Depression Scale in screening for major depressive episodes: a cross-sectional population-based study. BMC Res Notes. 2017;10(1):57.
- Kim DR, Epperson CN, Weiss AR, Wisner KL. Pharmacotherapy of postpartum depression: an update. Expert Opin Pharmacother. 2014;15(9):1223–1234.
- O’Hara MW, Engeldinger J. Treatment of postpartum depression: recommendations for the clinician. Clin Obstet Gynecol. 2018;61(3):604–614.
- Hantsoo L, Ward-O’Brien D, Czarkowski KA, et al. A randomized, placebo-controlled, double-blind trial of sertraline for postpartum depression. Psychopharmacology (Berl). 2014;231(5):939–948.
- Molyneaux E, Telesia LA, Henshaw C, et al. Antidepressants for preventing postnatal depression. Cochrane Database Syst Rev. 2018 Apr 18;4:CD004363.
- Sockol LE. A systematic review of the efficacy of cognitive behavioral therapy for treating and preventing perinatal depression. J Affect Disord. 2015;177:7–21.
- Miniati M, Callari A, Calugi S, et al. Interpersonal psychotherapy for postpartum depression: a systematic review. Arch Womens Ment Health. 2014;17(4):257–268.
- Milgrom J, Gemmill AW, Ericksen J, et al. Treatment of postnatal depression with cognitive behavioural therapy, sertraline and combination therapy: a randomised controlled trial. Aust N Z J Psychiatry. 2015;49(3):236–245.
- Swanson LM, Burgess HJ, Zollars J, Todd Arnedt J. An open-label pilot study of a home wearable light therapy device for postpartum depression. Arch Womens Ment Health. 2018;21(5):583–586.
- Cameron EE, Hunter D, Sedov ID, Tomfohr-Madsen LM. What do dads want? Treatment preferences for paternal postpartum depression. J Affect Disord. 2017;215:62–70.
- Lee JY, Knauer HA, Lee SJ, et al. Father-inclusive perinatal parent education programs: a systematic review. Pediatrics. 2018;142(1). pii: e20180437.