
 by Jeffrey Guina, MD, and Cathryn Guina, BSN, RN, CNRN
by Jeffrey Guina, MD, and Cathryn Guina, BSN, RN, CNRN
Dr. Jeffrey Guina is with the Department of Psychiatry, Wright State University Boonshoft School of Medicine in Dayton, Ohio, and the 88th Medical Group, Wright-Patterson Medical Center, Wright-Patterson Air Force Base in Ohio. Ms. Cathryn Guina is with the Neuroscience Institute Stroke Program, Kettering Memorial Hospital in Kettering, Ohio.
Innov Clin Neurosci. 2017;15(1–2):45–48.
FUNDING: No funding was provided for this article.
DISCLOSURES: The authors report no conflicts of interest relevant to the content of this article.
ABSTRACT: While post-stroke depression (PSD) is a common sequelae of stroke, many stroke survivors also have expressive aphasia (i.e., the inability to produce spoken or written language), which limits or prevents treating depression with talk psychotherapy. Unlike most psychotherapy modalities, eye movement desensitization and reprocessing (EMDR) does not require extensive verbal communication to therapists, which might make EMDR an ideal treatment modality for aphasic patients with mental health concerns. The authors present the first known case reporting EMDR in aphasia, describing the treatment of a 50-year-old woman with a history of depression following a left middle cerebral artery stroke. Left frontal lobe strokes are independently associated with both PSD and expressive aphasia. EMDR began two years following the stroke, at which point the patient continued to have persistent expressive aphasia despite previously completing more than a year of speech therapy. Using the Blind to Therapist Protocol, EMDR successfully led to improvement in depressive symptoms and, surprisingly, improvement in aphasia. This case report suggests that EMDR might be beneficial for those with mental health concerns who have expressive communication impairments that might prevent treatment with other psychotherapy modalities. We discuss potential challenges and technical workarounds with EMDR in aphasia, we speculate about potential biopsychosocial explanations for our results, and we recommend future research on EMDR for PSD and other mental health concerns in the context of aphasia, as well as possibly for aphasia itself.
KEYWORDS: Stroke, aphasia, depression, EMDR, psychotherapy
INTRODUCTION
Among stroke survivors, 35 percent develop expressive and/or receptive aphasia, 30 percent develop post-stroke depression (PSD), and seven percent complete suicide.[1,2] Treating PSD is important because of increased risks for all-cause mortality, suicide, recurrent stroke, and worse neurological recovery.[2–7] While studies have indicated that antidepressants and psychotherapy are effective for PSD,[2,3,8] psychotherapy options are very limited for those with comorbid aphasia. Only a few studies/cases have been reported demonstrating positive results with behavioral therapy,[9] counseling[10] and family therapy.[11] Although the ability to communicate is generally considered a prerequisite for psychotherapy, verbal expression of information is not necessary for eye movement desensitization and reprocessing (EMDR) to be successful.[12]
EMDR is a psychotherapy that uses, among other techniques, alternating bilateral stimulation (BLS; e.g., eye movement, auditory, tactile) while patients internally attend to memories, emotions, cognitions, images, and bodily sensations. The blind to therapist (B2T) protocol[13] was developed for those unwilling/unable to describe memories during EMDR due to control, shame/embarrassment, cultural reasons, or language barriers. Though EMDR is effective for depression,[14–16] PubMed, PsycINFO, EMDRIA, and Ingenta Connect searches did not reveal any articles about EMDR in those with comorbid aphasia. We aimed to determine if our patient with PSD could benefit from EMDR despite severe expressive aphasia.
CASE REPORT
Participant. Written consent for this case report was obtained from the patient, who has been anonymized. “Philomela,” a 50-year-old right-handed woman with depression onset after stroke—and no evidence of prior psychiatric symptoms—suffered a left middle cerebral artery stroke resulting in hemiplegia and Broca’s aphasia (both implicating frontal lobe). Based on formal speech pathology assessment, she had severely impaired functional spontaneous language skills and written expression and moderately impaired reading and auditory comprehension. Meeting a certified speech-language pathologist 2 to 3 times weekly for seven months, her comprehension difficulties were nearly resolved. However, severe expressive deficits, being wheel-chair bound, anhedonia, and hopelessness led to social withdrawal and dropping out of speech, physical, and occupational therapies.
At her first psychiatric appointment—10 months post-stroke—Philomela was dysphoric and mostly used head nods/shakes to communicate with rare “yes”/“no” answers. We discussed diet, exercise, social activity, antidepressants, stroke support groups, and restarting stroke-related therapies. Escitalopram was prescribed because serotonergic antidepressants have been shown to improve PSD and post-stroke neurological recovery2 and low anti-cholinergic effects, which can potentially worsen neurological deficits compared to others.[17,18] Within weeks, Philomela resumed socializing and stroke-related therapies (including 7 more months of speech therapy, which resulted in some improvement in using a speech-generating device), but she continued to experience severe expressive aphasia. However, depression insidiously returned, culminating in a serious suicide attempt. Bupropion was started to augment escitalopram and because it lacks anticholinergic activity. This resulted in modest improvements. Additional therapies (e.g., psychotherapy, music, art, yoga, cognitive rehabilitation) were recommended but difficult to find or inappropriate due to limitations, so EMDR was suggested.
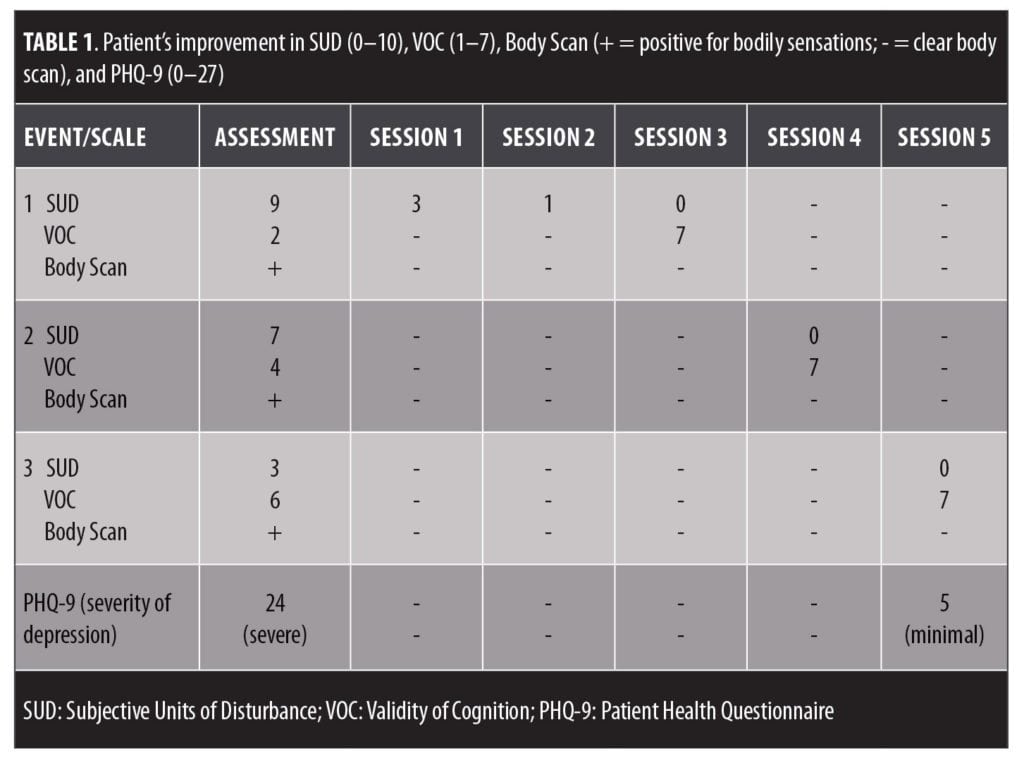
Measures. All measures were clinician-administered due to aphasia. Depression severity was assessed using the Patient Health Questionnaire (PHQ-9), a commonly used 0 to 27 scale. EMDR’s standard assessment tools assessed progress: Subjective Units of Disturbance (SUD), a 0 to 10 scale with 10 indicating the worst distress; Validity of Cognition (VOC), a 1 to 7 scale with 7 indicating the strongest belief in a positive cognition; and Body Scan, which systematically attends to body parts for sensations.
Treatment. EMDR began 24 months post-stroke with weekly one-hour sessions. The first three sessions involved history-taking, preparation/education, and assessment (identifying images, positive/negative cognitions, emotions, VOC, SUD, and bodily sensations associated with target memories). These were greatly aided by her husband (whom she requested to be at all sessions) and with lists of cognitions/emotions. She selected three target events to process using desensitization (reducing distress with sets of BLS) with cognitive interweaves (brief clinician statements/questions between BLS), and installation (enhancing positive self-referencing beliefs using BLS).
Using a biopsychosocial formulation based on history-taking/assessment, the clinician generally could hone guesses that Philomela would confirm/deny. It was important not to rush offering alternatives even after an emotion/cognition was agreed with (i.e., she would often identify better words to describe what she was feeling/thinking). Nevertheless, occasionally Philomela’s thoughts could not be communicated/guessed. Two target memories were identified—stroke and suicide attempt—but a third event remained elusive, even after listing potential traumas/stressors and administering the Adverse Childhood Experience Questionnaire.[19] The unidentified event was narrowed to occurring “25 years ago,” which became its cue phrase. It was harder to guess related cognitions/emotions, but she acknowledged having the words in her mind that could be cued (e.g., “negative belief”).
As recommended in B2T, where the therapist cannot assess “change,” Philomela was taught the nature of change in EMDR and was instructed to use nods/shakes or yes/no similar to a case report involving stuttering.12 Desensitization was initially difficult: she required frequent reminders about the nature of change, feedback was often stalled by aphasia, and it became clear that high numbers of rapid BLS passes were necessary for change (she reported no change with too slow/few, 50 were generally sufficient following positive changes, but 100 were needed otherwise). When she could not verbalize feedback, she was reassured that EMDR can work even with internal processing without the clinician knowing specifics. Gradually, the process became more familiar, and the clinician became more attuned, leading to better guesses. A workable pattern developed in which the following steps were repeated again and again:
- BLS
- Deep breath
- Time to respond
- If unable to verbalize, “is it a feeling?… thought?… image?… or body sensation?”
- “Is it positive or negative?”
- Clinician guesses
- Whether or not the change could be identified, BLS resumed +/- cognitive interweave.
Results. Table 1 displays how the rate of progress improved exponentially, resulting in improved depression. When processing stalled, cognitive interweaves became very effective (e.g., “Can someone require a lot of help and still be a worthwhile person?”; “If your child was in a wheelchair, would you still think they were a worthwhile person?”; “Even if your stroke symptoms never improve can you still live a good life?”; “Can you have physical limitations and still be loved and important to others?”). Philomela often gave surprisingly negative responses to cognitive interweaves, but with continued BLS and returns to target, positive changes eventually occurred and became sustained. At four months post-EMDR, depression remained remitted with her return to a full social life and enjoyable activities, reinventing her life within her physical/speech limitations.
While our target had been depression, there were subjective (i.e., reported by patient, family, and clinician) improvements in aphasia, initiation, and verbal apraxia. She started using multisyllabic words (e.g., “heaviness,” “positive,” “emotional,” and “contentment,” the latter being said without first being said by the clinician, astounding herself and her husband), verbalized things the clinician had been unable to guess (e.g., the third event) and, in her last session, she said her husband’s name for the first time in two years. He admitted being skeptical of EMDR originally but happily said, “she made more progress in two months with this than in over a year of speech therapy.”
DISCUSSION
In Greek mythology, Philomela was raped and her tongue was cut out to keep her silent. Rendered unable to speak, she wove a tapestry of her story and was turned into a nightingale by the gods to escape her tormentor (while male nightingales sing, females are mute). Like the Greek Philomela, our case involved a woman who was rendered unable to speak. Through EMDR, she was able to process her story nonverbally and was able to take flight into a worthwhile life.
While known to be effective for depression, we can only speculate how EMDR helped this specific patient. EMDR activates the frontal lobe,[20,21] which might explain its utility for PSD and, perhaps, the surprising improvement in aphasia. Stress-induced deactivation in Broca’s area has been repeatedly implicated in the difficulty that trauma survivors have when discussing traumas.[22–25] It is conceivable that EMDR and antidepressants enhanced frontal lobe activation and neuroplasticity.
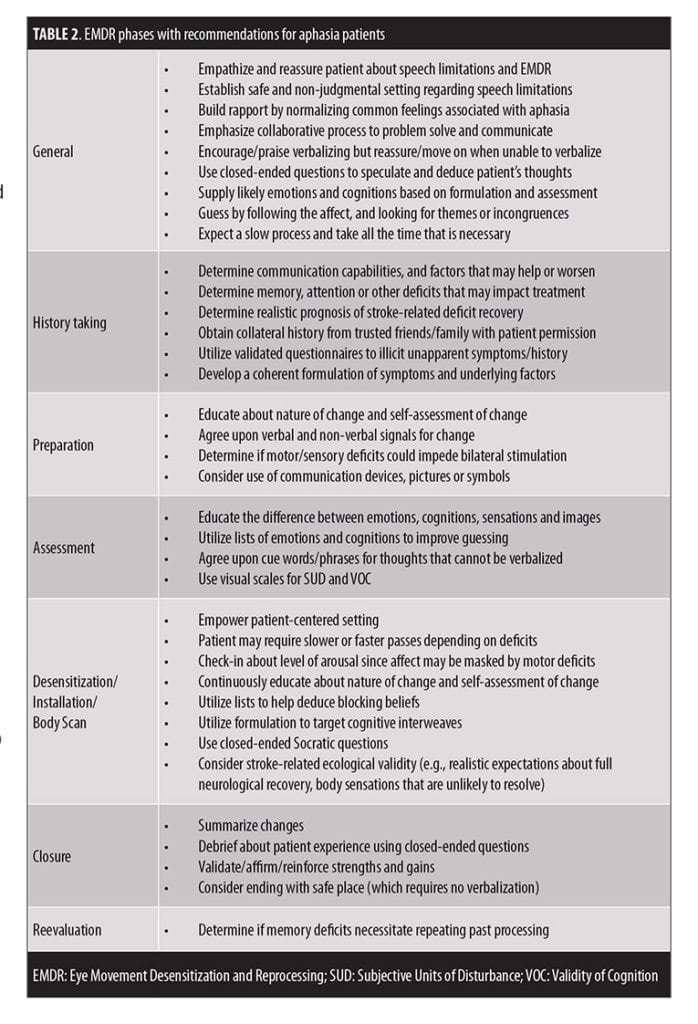
Table 2 summarizes considerations for EMDR with aphasia. Anticipatable issues include regularly explaining change, trouble identifying cognitions, and more time needed in all phases. While initially distracting, the husband’s presence was likely beneficial as he provided collateral information, improved guesses, and was able to bear witness to her struggles and successes. Helpful preparation included consultation, literature searches, and organizing visual scales and lists of emotions/cognitions. It should be noted that our patient had only expressive aphasia, as her comprehension issues had been successfully treated by a speech-language pathologist; EMDR might lack utility for those with receptive aphasia.
As a single case report, further research is required to determine EMDR efficacy for mental disorders with comorbid aphasia. Not expecting speech improvements, we did not use objective measures as we did with depression, so the aphasia findings are anecdotal. It is possible that aphasia seemed to improve because the therapist became more familiar with her, or only secondary to reduced depression (e.g., perhaps it was not the “aphasia” that improved but rather the patient’s ability to connect with others due to remission of depression), or that symptoms improved because of the husband’s presence (e.g., his attention helped lift her depression), but the clinical observations warrant further research. Irrespective of aphasia, this study indicates that EMDR can be effective for PSD despite comorbid aphasia and that these patients have more treatment options than previously thought.
CONCLUSION
This is the first reported case demonstrating that EMDR can be effective for depression, even in those with severe expressive aphasia. In our case, there was no reluctance to disclose information, simply a neurological inability to do so. Through preparation, patience, perseverance, and plasticity (clinician flexibility, though perhaps also neuroplasticity), the patient’s PSD gradually improved, and she was able to reinvent her life within her limitations.
ACKNOWLEDGMENTS
The authors gratefully acknowledge Eugene Schwartz, E.C. Hurley, and Mark Hubner for providing consultation during patient care.
REFERENCES
- Dickey L, Kagan A, Lindsay MP, et al. Incidence and profile of inpatient stroke-induced aphasia in Ontario, Canada. Arch Phys Med Rehabil. 2010;91:196–202.
- Byars JA, Jorge RE. Neuropsychiatric sequelae of stroke: issues and implications for clinicians. Psychiatr Times. 2015;32(3):36G–H.
- Code C, Hermann M. The relevance of emotional and psychosocial factors in aphasia to rehabilitation. Neuropsychol Rehabil. 2003;13(1/2):109–132.
- Code C, Hemsley G, Herrmann M. The emotional impact of aphasia. Semin Speech Lang. 1999;20:19–31.
- Code C. The quantity of life for people with chronic aphasia. Neuropsychol Rehabil. 2003;13(3):379–390.
- Joseph R. Frontal lobe psychopathology: mania, depression, confabulation, catatonia, perseveration, obsessive compulsions, and schizophrenia. Psychiatry. 1999;62(2): 138–172.
- Kouwenhoven SE, Kirkevol M, Engedal K, Kim HS. Depression in acute stroke: prevalence, dominant symptoms and associated factors. A systematic literature review. Disabil Rehabil. 2011;33(7):539–556.
- Ramasubbu R. Therapy for prevention of post-stroke depression. Expert Opin Pharmacother. 2011;12(14):2177–2187.
- Thomas SA, Walker MF, MacNiven JA, et al. Communication and low mood (CALM): A randomized controlled trial of behavioural therapy for stroke patients with aphasia. Clin Rehabil. 2013;27(5):398–408.
- Cunningham R. Counselling someone with severe aphasia: an explorative case study. Disabil Rehabil. 1998;20(9):346–354.
- Nichols F, Varchevker A, Pring T. Working with people with aphasia and their families: An exploration of the use of family therapy techniques. Aphasiology. 1995;10(8):767–781.
- Blore DC, Holmshaw EM, Swift A, et al. The development and uses of the “blind to therapist” EMDR protocol. J EMDR Practice Research. 2013;7(2):95–105.
- Blore DC, Holmshaw EM. EMDR “blind to therapist protocol.” In: Luber M (ed). Eye movement desensitization and reprocessing: EMDR scripted protocols basic and special situations. New York, NY: Springer;2009:233–240.
- Hase M, Balmaceda UM, Hase A, et al. Eye movement densitization and reprocessing therapy in the treatment of depression. Brain Behav. 2015;5(6):e00342. doi: 10.1002/brb3.342
- Hofmann A, Hilgers A, Lehnung M, et al. J EMDR Practice Research. 2014;8:103–112.
- Moghadam MB, Moghadam AB, Salehian T. Efficacy of eye movement desensitization and reprocessing (EMDR) on depression in patient with myocardial infarction (MI) in a 12-month follow up. Iran J Crit Care Nurs. 2015;7(4):221–226.
- Cole MG, Elie LM, McCusker J, et al. Feasibility and effectiveness of treatments for depression in elderly medical inpatients: a systematic review. Int Psychogeriatr. 2000;12(4):453–461.
- Stahl SM. Stahl’s Essential Psychopharmacology, fourth edition. New York, NY: Cambridge;2013.
- Anda RF, Butchart A, Felitti VJ, Brown DW. Building a framework for global surveillance of the public health implications of adverse childhood experiences. Am J Prev Med. 2010;39:93–98.
- Hull AM. Neuroimaging findings in post-traumatic stress disorder. Br J Psychiatry. 2002;181(2):102–110.
- van der Kolk BA. Posttraumatic stress disorder and the nature of trauma. Dialogues Clin Neurosci. 2000;2(1):7–22.
- Rauch SL, van der Kolk BA, Fisher RE, et al. A symptom provocation study of post-traumatic stress disorder using positron emission tomography and script driven imagery. Arch Gen Psychiatry. 1996;53(5):380–387.
- Shin LM, McNally RJ, Kosslyn SM, et al. A positron emission tomographic study of symptom provocation in PTSD. Ann N Y Acad Sci. 1997;821:521–523.
- Shin LM, McNally RJ, Kosslyn SM, et al. Regional cerebral blood flow during script-driven imagery in childhood sexual abuse-related PTSD: A PET investigation. Am J Psychiatry. 1999;156(4):575–584.
- Cottraux J, Lecaignard F, Yao SN, et al. Magneto-encephalographic (MEG) brain recordings during traumatic memory recall in women with post-traumatic stress disorder: a pilot study. Encephale. 2015;41(3):202–208.