
 by Arshya Vahabzadeh, MD; Ned Sahin, PhD; and Amir Kalali, MD
by Arshya Vahabzadeh, MD; Ned Sahin, PhD; and Amir Kalali, MD
Dr. Vahabzadeh is Director of Digital Health, Brain Power, in Cambridge, Massachusetts; Instructor in Psychiatry, Harvard Medical School in Cambridge, Massachusetts; and Innovation Officer at Massachusetts General Hospital Psychiatry Academy in Boston, Massachusetts. Dr. Sahin is Chief Science Officer at Brain Power and Associate in Psychology at Harvard University in Cambridge, Massachusetts; and Dr. Kalali is Global Head of the Neuroscience Center of Excellence at Quintiles and Professor of Psychiatry at the University of California, San Diego, California.
Innov Clin Neurosci. 2016;13(5–6):16–20.
Funding: No funding was provided for the preparation of this article.
Financial disclosures: Dr. Vahabzadeh is Director of Digital Health and Dr. Sahin is Chief Science Officer at Brain Power, which is a digital mental health company in Cambridge, Mass. Dr. Kalali has no conflicts of interest relevant to the content of this article.
Abstract: Suicide continues to be a leading cause of death and has been recognized as a significant public health issue. Rapid advances in data science can provide us with useful tools for suicide prevention, and help to dynamically assess suicide risk in quantitative data-driven ways. In this article, the authors highlight the most current international research in digital suicide prevention, including the use of machine learning, smartphone applications, and wearable sensor-driven systems. The authors also discuss future opportunities for digital suicide prevention, and propose a novel Sensor-driven Mental State Assessment System.
Key words: Mhealth, suicide, depression, technology, apps, machine learning, data science, wearables, digital health
This column series explores the emerging field of digital medicine and how innovative technology can improve patient outcomes in the field of neuroscience.
Introduction
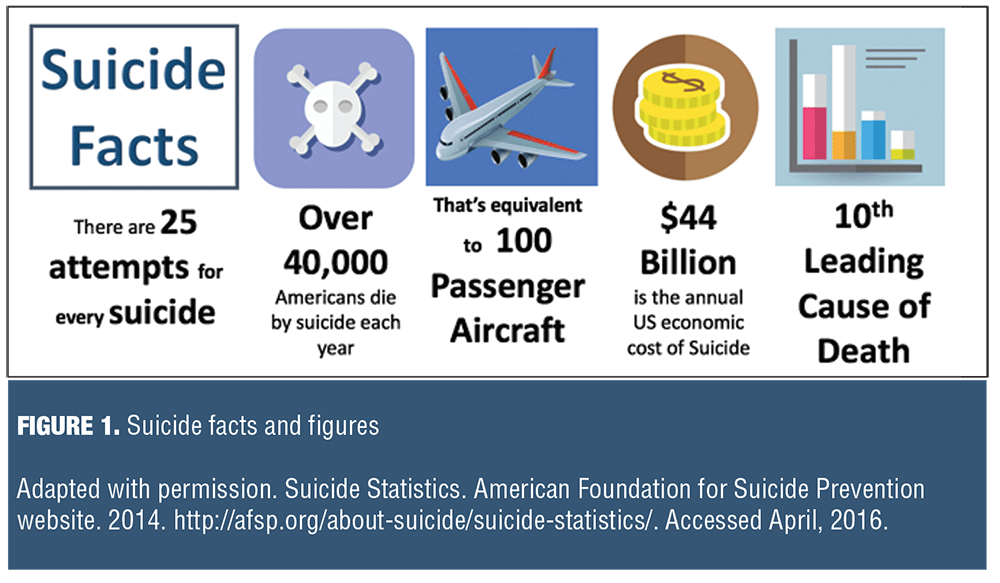
Suicide is the second leading cause of death in people aged 15 to 34 years and is a top 10 cause of death across all age groups in the United States (Figure 1).[1–3] While there have been huge advances in reducing death from conditions such as cancer and human immunodeficiency virus infection/ acquired immune deficiency syndrome (HIV/AIDS), the rate of suicide has barely changed in the last 50 years.
Although some people may view suicide as being less of a “medical” condition than diseases like cancer or HIV/AIDS, we do know that the vast majority of people who die by suicide have depression or another treatable brain disorder.[4]
Medication and psychotherapy have been used to treat these underlying disorders in suicidal patients, and new medications are being explored and developed specifically to address suicidality (e.g., ketamine[5]), which may aid in suicide prevention. Additionally, through the collection and analysis of large amounts of population and/or patient data, we may be able to produce a technology that can digitally identify high-risk individuals and suicidal behavior.
Leveraging technology in this manner has not been lost on key decision makers. Recently, the White House hosted the Partnerships for Suicide Prevention event, with the mission statement of “Using Data to Strengthen Mental Health Awareness and Suicide Prevention.” The White House also organized a five-city suicide prevention “hackathon” that brought together data scientists, innovators, designers, and next-gen technologists from several different organizations. They were challenged to collaborate and develop products, tools, or data analysis on suicide prevention.[6]
Death by suicide is a complex situation and is usually preceded by suicidal thoughts, plans, and attempts.[7] Dramatic advances in data science and wearable technology may provide us with new avenues to recognize suicidal behavior, prevent suicide, and save lives. .
Predicting Suicide using Data Science
One of the key roles of a psychiatrist is to assess the risk of suicide in his or her patients. While we know of many risk factors for suicide, psychiatrists have to rely on clinical acumen to assess suicide risk. This assessment carries with it a degree of subjectivity, and we have not yet been able to create an automated system to model and predict suicide risk objectively. Suicide risk is also highly fluid, with the potential for rapid fluctuations based on biological, social, and psychological factors. Additionally, suicide risk has both chronic and acute elements: someone may be chronically at high risk of suicide, although a more immediate life event may rapidly escalate that risk further. People who are at relatively low risk may also become at high imminent risk due to an acute life event. While negative life events and stress have been linked to suicide, some have argued that even neutral or positive life events can result in stress and an increased suicide risk. The impact of positive life events on suicide risk appears to be complicated and poorly elucidated at present.[8]
By collecting and analyzing large amounts of population and/or patient data, technology that digitally predicts suicides could help us to objectively quantify 1) the general impact of each of the many different risk factors and how they interact, 2) the specific risk profile of a given individual, and 3) an individual’s instantaneous risk at any given moment with consideration of any newly acquired information. Such a technology would help us more effectively target our limited resources across a much larger population. While these prospective interventions may seem optimistic, a range of research is giving us hope that they could be possible.
Research, from Soldiers to Students
The mental health needs of our military personal are enormous, and our soldiers and veterans are a particularly high-risk group for suicide, so it makes sense for researchers to concentrate their efforts on this population. One study analyzed over 40,000 soldiers who required psychiatric hospitalization, and by using a specialized machine learning system, the researchers managed to devise a predictive suicide risk algorithm.9 The algorithm succeeded in that over 50 percent of the soldiers who committed suicide in the following year were in the top five percent it had predicted. This was based simply on factors like gender and listed criminal/medical records—they didn’t include any additional behavioral or clinical data from the subsequent year. In theory, using a more refined version of this approach, applied to the general public, could allow us to pinpoint the highest-risk individuals and deliver suicide prevention services to them first, customized to their specific risk profiles. This could save many more lives and deploy our nation’s budget-stretched psychiatric services in a highly efficient and more cost-effective way.
Researchers outside of the United States have also been exploring data-science driven approaches to suicide prevention. South Korean researchers have studied another high-risk population—teenage students—and their attempts are somewhat urgent given that South Korean has one of highest suicide rates in the world. The overall rate of suicide in South Korea is more than double the rate in the United States. While men have higher rates of suicide in both countries, women in South Korea have suicide rates that are 3.5 times higher than women in the United States. The South Korean researchers discovered that almost 10 percent of their middle- and high-school students have attempted suicide. Instead of using traditional statistical methods, the authors used a data mining technique to understand the risk factors that lead to a suicide attempt.[9] In other words, instead of trying to prove or disprove a particular proposed theory, the authors used data mining analysis to attempt to identify every possible interaction between a huge range of different variables (i.e., big data). They found that in students who were very depressed, the biggest factor predicting a suicide attempt was delinquency, especially in female students. In contrast, of those students who had only a few symptoms of depression, lower levels of intimacy with their family members was the biggest risk factor. In children who were not depressed, stress, such as from falling academic performance, was the biggest risk factor for a suicide attempt. These findings are fascinating, as they allow us to quantitatively understand how individual risk factors can affect groups of individuals differently.
Computerized Speech and Facial Emotions Analysis
Speech and facial emotions may also provide a window into detecting suicidal thinking. Through the use of computerized speech analysis, researchers are able to find differences in how depressed and/or suicidal people talk. People who become suicidal may have differences in the sound frequency of their speech, either going from high frequency to low frequency or vice-versa. Research has also shown that people with depression exhibit a reduced acoustic range to their speech.[11]
Other researchers are using computerized real-time facial emotion monitoring to also detect subtle changes in the facial expressions of people with suicidal thoughts. For example, researchers at University of Massachusetts and Affectiva are attempting to identify people with suicidal thoughts based on how they respond to various video vignettes. They are using a specialized computer program to analyze facial expressions, in addition to measuring body measurements such as skin conductance and heart rate. They hope to demonstrate differences in how people with suicidal thoughts react emotionally and physically to various videos in comparison to those without. Such research could allow us to develop a rapid way to assess suicidality, especially in high risk individuals who may not verbally disclose the presence of suicidal thoughts or plans.[12]
Psychiatrists and other mental health clinicians are routinely trained in performing a mental state examination (MSE), a systematic, but subjective, method of assessing and documenting a person’s physical and mental presentation.[13] The history and MSE are recognized as being some of the most important diagnostic and assessment tools for a clinical psychiatrist.[13] The MSE includes an assessment of an individual’s mood, speech, thought patterns, and behavior. We propose the development of a digital mental state examination (dMSE) that assesses a patient’s presentation by utilizing a range of technologies including motion tracking, natural language processing, and speech analysis to produce quantitative, objective data that may be superior to the subjective reporting of the standard clinical MSE.
Can Computerized Therapy and Smartphone Apps Help?
There has been some emerging evidence to suggest that computerized suicide prevention approaches may also be useful; an example is the use of automated cognitive behavioral therapy (CBT). Automated CBT can deliver a course of this particular type of talk therapy without the involvement of a human therapist. Unfortunately, while there is some evidence to suggest the utility of such approaches in affective disorders, the evidence for its use in suicide is far more limited.[14]
There is even less research available on smartphone applications (apps) for suicide. Some would argue that smartphones and other wearable devices maybe ideal platforms to assess and even treat mental health conditions. The research team at Brain Power recently conducted a review of suicide-related smartphone apps, and their conclusions were quite worrying. The vast majority of apps were little more than checklists of symptoms or resources. Some apps contained information that could be potentially harmful or may worsen a person’s condition. In general, these apps did not leverage the complex inbuilt sensors and hardware capabilities of smartphones to collect behavioral data or incorporate any significant data analysis. Prior research on suicide-related apps supports our team’s findings, with up to 13 percent of apps containing content that could be potentially harmful, and over half having no interactive features.[14] A recent systemic review of suicide and self-harm apps highlighted similar concerns.[15] This suggests that we are at the very beginning of leveraging technology that can be delivered via an app platform. This may change as large technology companies are getting more interested in impacting healthcare.
Researchers have created a suicide prediction system that combines data from mood-focused smartphone apps, and also genetic blood tests (biomarkers).[16] These researchers have found that by combining the results of both of these approaches, they can predict suicidality and also hospitalizations from suicide attempts. Interestingly, the smartphone apps ask participants questions about their mood and life, but did not directly ask about suicidality. This contrasts to the current standard of clinical care, where directly asking about suicidal ideation is essential. The notion that people will be promoted to commit suicide through such questioning has long been dismissed. The researcher’s system has been found to predict suicidality in women, a historically understudied group. Despite this research, it appears that considerably more research and development needs to be done before mental health apps play a significant role in suicide prevention.[16]
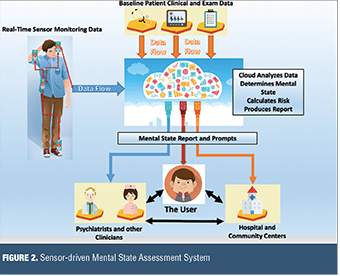
We also propose that there is potential to detect and monitor suicidal ideation through the use of cloud computing to generate a personalized computer model of an individual’s real-time emotional state (Figure 2). Some researchers have proposed some basic elements of this technique, such as using interconnected non-invasive sensors to monitor electro-dermal activity and electroencephalogram (EEG).[16] We believe that a more robust model would leverage a combination of physiologic measurements from bio-sensors, proxy measurements of social interaction from smartphone sensors, and a patient’s baseline demographic and clinical data. Through the use of data analytics and cloud computing, we believe that a personalized real-time mental state and suicide risk model can be developed for the user of such a system. This system would be able to give real-time feedback to the user, psychiatrists, and other clinicians, and also the wider health system. Such a system could allow for remote monitoring, early identification of suicidal states, and beneficial changes in treatment plans. Privacy and confidentially concerns will be paramount in the development of such systems given the sensitive nature of the collected data, and users will have to carefully weigh up the risks and benefits of these systems before consenting to their use.
Final Thoughts
Will a new generation of connected devices help us detect and prevent suicide? It may seem like science fiction to some. Today’s multitude of wireless devices may help us finally improve the bleak statistics and subjective clinical approaches we’ve utilized thus far in suicide prevention. Yet we must immerse ourselves in the population to see the nuances of suicidality. For instance, the most at-risk, or those at their riskiest moments of life, may never charge their phones nor motivate to check in with an online service, thus passive monitoring that doesn’t require batteries must be a part of any solution. There has been an increase in research that focuses on predicting and understanding suicide using new technologies, yet there remains a considerable need for caution, given the severity of any potential oversight or error. Many of these preliminary results are positive and give us hope that these initiatives may end up being an important part of our suicide prevention armamentarium. Mental health clinicians will continue to play a central role in suicide prevention, and early use of these technologies will augment the work of human clinicians, not replace them. It is also imperative that people with psychiatric illness, including suicidal thoughts, are actively involved in the design and development of these technologies. This approach will ensure that the technology has a suitable user interfaceand results in high levels of user engagement, thus is acceptable in real-world situations and is effective.
Acknowledgement
The authors would like to acknowledge the input of Sophie Katz, Neuroscience, Duke University.
References
1. Suicide: facts at a glance. Centers for Disease Control and Prevention website. 2015. http://www.cdc.gov/violenceprevention/pdf/suicide-datasheet-a.pdf. Accessed April, 15, 2016.
2. Leading causes of death. Centers for Disease Control and Prevention website. April 27, 2016. http://www.cdc.gov/nchs/fastats/leading-causes-of-death.htm. Accessed April, 15, 2016.
3. Suicide statistics. American Foundation for Suicide Prevention website. 2014. http://afsp.org/about-suicide/ suicide-statistics/. Accessed April 15, 2016.
4. Bertolote JM, Fleischmann A. Suicide and psychiatric diagnosis: a worldwide perspective. World Psychiatry 2002;1:181–85.
5. DiazGranados N, Ibrahim L, Brutsche N, et al. Rapid resolution of suicidal ideation after a single infusion of an NMDA antagonist in patients with treatment-resistant major depressive disorder. J Clin Psychiatry. 2010;71(12):1605–1611.
6 Patil DJ, Honey K. Open data and innovation for suicide prevention: #MentalHealthHackathon. The White House website. December 9, 2015. https://www.whitehouse.gov/ blog/2015/12/09/open-data-and-innovation-suicide-prevention-mentalhealthhackathon. Accessed April, 2016
7. Klonsky ED, May AM, Saffer BY. Suicide, suicide attempts, and suicidal ideation. Annual Rev Clin Psychol. 2016;12:307–330.
8. Cornette, M, Busch A. Stress and suicide , The Charles E. Kubly Foundation website. http://charlesekublyfoundation.org/resource-center/resource-articles/stress-and-suicide. 2016. Accessed April 15, 2016
9. Kessler RC, Warner CH, Ivany C, et al. Predicting suicides after psychiatric hospitalization in US Army soldiers: the Army Study to Assess Risk and Resilience in Service members (Army STARRS). JAMA (Psychiatry) 2015;72(1):49–57.
10. Bae SM, Lee SA, Lee SH. Prediction by data mining, of suicide attempts in Korean adolescents: a national study. Neuropsychiatr Dis Treat. 2015;11:2367–2375
11. Larsen ME, Cummins N, Boonstra TW, et al. The use of technology in suicide prevention. Presented at 37th Annual International Conference of the Engineering in Medicine and Biology Society. August 26–29, 2015. Milan, Italy.
12. Vannoy S, Gable S, Brodt M, et al. Using affect response to dangerous stimuli to classify suicide risk. Presented at CHI 2016 Computing and Mental Health Workshop. San Jose, CA. 8 May 2016.
13. Brannon GE, Bienenfeld D, Talavera F, Schmetzer AD. History and mental status examination. Medscape website. 31 Mar, 2016. http://emedicine.medscape.com/article/293402-overview#a3. Accessed June 15, 2016.
14. Lai MH, Maniam T, Chan LF. Ravindran AV. Caught in the web: a review of web-based suicide prevention. J Med Internet Res. 2014;16(1):30.
15. Larsen ME, Nicholas J, Christensen H. A Systematic assessment of smartphone tools for suicide prevention. PLoS One. 2016;11(4):e0152285.
16. Levey DF, Niculescu EM, Le-Niculescu H, et al. Towards understanding and predicting suicidality in women: biomarkers and clinical risk assessment. Mol Psychiatry. 2016;21(6):768–785.
17. Alam MGR, Cho EJ, Huh EN, Hong CS. Cloud based mental state monitoring system for suicide risk reconnaissance using wearable bio-sensors. Presented at the 8th International Conference on Ubiquitous Information Management and Communication. 9–11 Jan 2014. Siem Reap, Cambodia.