
 by Muhammad Hassan Majeed, MD; Ali Ahsan Ali, MD; Hafiza Ayesha Khalil, MD; Douglas Bacon, MD; and Hafiz Muhammad Imran, MD
by Muhammad Hassan Majeed, MD; Ali Ahsan Ali, MD; Hafiza Ayesha Khalil, MD; Douglas Bacon, MD; and Hafiz Muhammad Imran, MD
Dr. Majeed is with the Department of Anesthesiology and Critical Care Management, Johns Hopkins Hospital in Baltimore, Maryland. Dr. Ali is with the Department of Psychiatry, Icahn School of Medicine at Mount Sinai (Elmhurst) in Queens, New York. Dr. Khalil is with Good Samariton Hospital in Lebanon, Pennsylvania. Dr. Bacon is with the Department of Anesthesiology, The University of Mississippi Medical Center School of Medicine in Jackson, Mississippi. Dr. Imran is with Providence VA Medical Center/Rhode Island Hospital in Providence, Rhode Island.
Funding: No funding was provided.
Disclosures: The authors have no conflicts of interest relevant to the content of this article.
Abstract: Background: The incidence rates of heart failure (HF) and chronic pain increase with age. In the geriatric population, both disorders often coexist and pose a challenge to clinicians in treating them simultaneously. Methods: We conducted an online literature search for reports of the heart failure effects of pharmacological treatments for chronic pain. Results: Topical pain medications are favored agents because of their efficacy, tolerability, and favorable side-effect profile. Acetaminophen is a preferred oral medication for the treatment of pain in patients with HF. Due to deleterious effects including HF, the long-term use of oral nonsteroidal anti-inflammatory drugs and gabapentinoids are discouraged. Conclusion: Prescribers should thoroughly consider the risk–benefit ratio and individual patient-risk profile before instituting pharmacological treatment for chronic pain in patients with HF.
Keywords: chronic heart failure, chronic pain, heart failure, nonsteroidal anti-inflammatory drugs (NSAIDs), pharmacology
Innov Clin Neurosci. 2019;16(11–12):25–27
Heart failure (HF) is a complex clinical syndrome resulting from impaired ventricular filling and/or ejection of blood. Its incidence increases with age from approximately 20 per 1,000 persons between 65 to 69 years of age to more than 80 per 1,000 persons older than 85 years of age.1 In the United States, more than 25 million adults suffer from chronic pain, and its prevalence grows with increasing age.2 When HF and chronic pain coexist, they pose a unique management challenge to clinicians. Many medications used to treat chronic pain might interfere with the management of HF. Inadequate pain control might worsen the quality of life and limit the ability to perform exercise—a proven therapeutic modality to decrease hospitalization and increase survival in patients with HF. There is limited data available to guide clinicians in prescribing pain medications for patients with the dual diagnosis of chronic pain and HF. In this review article, we present a systematic evaluation of pharmaceutical agents to manage chronic pain in patients with preexisting HF.
Methods
We searched the PubMed and Google Scholar electronic databases for relevant publications, using the following search terms: “chronic pain,” “osteoarthritis pain,” “nociceptive pain,” “neuropathic pain,” and “psychopharmacology” or “medications,” and “heart failure” or “cardiac failure.” Only original and human studies were selected for this review. No restrictions were applied.
Henceforth, we present a review of HF effects of the medications used for the treatment of neuropathic and nociceptive pain.
Neuropathic pain. Neuropathic pain is initiated or caused by a primary lesion or dysfunction in the nervous system. Its characteristic symptoms include heat hyperalgesia, cold allodynia, and mechanohyperalgesia.
Serotonin and norepinephrine reuptake inhibitors (SNRIs) are utilized in the treatment of both neuropathic and nociceptive pain. Venlafaxine and duloxetine are used often as an initial treatment for neuropathic pain, where they act as SNRIs and have moderate analgesic efficacy.3
Duloxetine has demonstrated its efficacy in reducing pain intensity in three placebo-controlled trials.4 SNRIs reduce levels of inflammatory markers such as inflammatory cytokines interleukin (IL)-1b, tumor necrosis factor-alpha, IL-6 and C-reactive protein in patients with depression. These inflammatory cytokines play an important role in the pathogenesis of HF.5 There have been no controlled studies to prove these benefits. Their other cardiovascular side effects include hypertension, palpitations, and tachycardia.
Tricyclic antidepressants (TCAs) modulate pain pathways by inhibiting norepinephrine and serotonin and enhancing transmission in inhibitory pathways in the central nervous system.3 The potential inflammation modulation by TCAs can be beneficial for patients of HF, but this effect has not been studied to date in humans. Higher doses of these medications require regular electrocardiogram monitoring to detect cardiac conduction problems.
Gabapentin and pregabalin are anticonvulsants frequently used in the management of neuropathic pain. They can lead to weight gain in 10 to 15 percent of patients with or without a history of congestive HF.6 A recent population-based study reported overall HF admission rates in patients aged 66 years or older using gabapentanoids was significantly higher (75 per 1,000 person-years) than in the general population (3–10 per 1,000 person-years).7 There was no significant difference between gabapentin and pregabalin use among HF admissions overall (0.5% vs. 0.4%) or in those with preexisting HF (4.1% vs. 4.0%). Gabapentinoids should be avoided in patients with a known diagnosis of HF.
Finally, in a recent Cochrane Review, the authors concluded that cannabis-based medications might be helpful for adults with neuropathic pain.8 The relation of these medications to HF is not known at this time.
Nociceptive pain arises from actual or threatened damage to non-neural tissue with the activation of nociceptors. To describe the pharmacological management in nociceptive pain disorders, we chose osteoarthritis (OA) pain as a model due to its high prevalence in the elderly. Moreover, patients with OA have an associated increased risk of cardiovascular disease, including particularly HF and ischemic heart disease.9 It is hypothesized that factors such as chronic inflammation, reduced mobility, and nonsteroidal anti-inflammatory drug (NSAID) use that are common in OA are also risk factors for developing cardiovascular disease.9
Due to a relatively better safety profile, acetaminophen is often used as the initial therapy for pain in OA.10 In therapeutic doses, it has no deleterious effect on the cardiovascular system. It is recommended as a preferred agent to treat pain in patients with HF.
NSAIDs are the most common analgesics available over the counter and are frequently used in the treatment of OA. NSAID usage can lead to HF exacerbations by increasing peripheral vascular resistance and decreasing renal perfusion, glomerular filtration rate, and sodium excretion in susceptible individuals.11 Current NSAIDS (both nonselective and selective cyclooxygenase inhibitors) users (drugs taken during the preceding two weeks) had a 20 percent higher risk of HF exacerbation than past users (drugs taken more than six months ago). Higher doses (>1.2 defined daily dose [DDD] equivalent) of naproxen, diclofenac, and etoricoxib increased the risk of HF exacerbation compared to low (<0.8 DDD) or moderate (0.8–1.2 DDD) doses of the same agents.11
Aspirin (ASA) in high doses (>250mg daily) can attenuate the effects of angiotensin-converting enzyme (ACE) inhibitors frequently used in the treatment of HF.12 Concomitant use of ASA and ACE inhibitors might require a dose adjustment for the latter.13
Topical NSAIDs have a similar efficacy and a better systemic side-effect profile for OA limited to a single or few joints.14 Topical NSAIDs should be recommended before initiating oral medications.
Capsaicin is reported to attenuate substance P and is integral in the perception of pain. There is moderate evidence to support the use of topical capsaicin in the treatment of OA pain.15 There are no studies or reports available that comment on the effects of capsaicin in patients with HF.
There is conflicting evidence about the efficacy of bisphosphonates in the management of OA. Grove et al16 reported an increased risk of HF in patients treated with first-generation bisphosphonates compared to the general population. In contrast, nitrogen-containing second-generation bisphosphonate alendronate significantly reduced the risk of HF compared to etidronate.16
Biologics are emerging treatments for OA, with promising preliminary data available. Tanezumab, fulranumab, and fasinumab are antinerve growth factor (anti-NGF) monoclonal antibodies that have proven to be efficacious in the treatment of chronic OA pain.17
NGF is also secreted from cardiac myocytes and is essential for the development, differentiation, and synaptic activity of the cardiac sympathetic nervous system. Low NGF levels have been reported in clinical and experimental models of HF.18 While the analgesic properties of anti-NGF are established, their clinical implications for patients with HF are not known.
Current guidelines discourage the use of opioids in the treatment of chronic OA pain due to a lack of long-term efficacy and the risk of overdose, addiction, or death. Even though morphine is commonly used to treat acute pulmonary edema, data describing the role of opioids in the management of dyspnea or pain in patients with HF are lacking. In a study, two doses of dihydrocodeine increased exercise tolerance, with an observed decrease in breathlessness in patients with HF demonstrating a potential beneficial role of opioids in HF.19
Discussion
Prescribers should thoroughly consider the risk–benefit ratio and individual patient-risk profile before instituting pharmacological treatment for chronic pain in patients with HF. To limit adverse events, medications should be restricted to the lowest effective dose and shortest duration. An interprofessional effort with a focus on nonpharmacological treatments, such as cognitive behavioral therapy, mindfulness, and yoga, should be encouraged as initial strategies to treat chronic pain.20–22
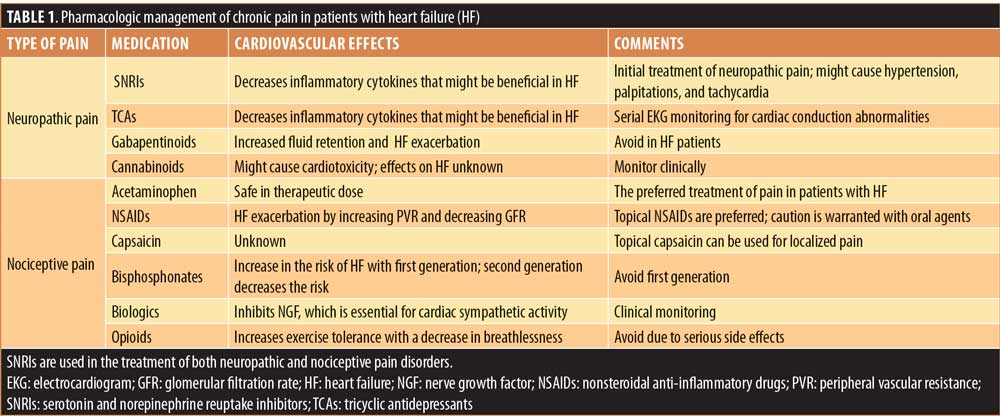
Topical medications, such as NSAIDs and Capsaicin, are favored agents because of their efficacy, tolerability, and favorable side-effect profile. Acetaminophen is a preferred oral medication for the treatment of pain in patients with HF. SNRIs, TCAs, opioids, and biologics have unique effects on the cardiovascular system including HF and clinicians should be mindful of their impact before initiating treatment. Due to deleterious effects including HF, the long-term use of oral NSAIDs and gabapentinoids is discouraged. These findings are summarized in Table 1.
The limitations of this review include excluding several medications used for the treatment of pain disorders, such as headache, orofacial pain, and other central pain disorders.
Conclusion
HF is a complex clinical syndrome, and the management of concomitant chronic pain can be challenging in these patients. Judicious use of pain medications can help to promote improved treatment outcomes and better quality of life among affected patients. More research is required to determine the specific risk of HF for each class of medication used to treat chronic pain, especially as reduced perfusion to organs, such as the kidney and liver might significantly impact the metabolism and the elimination of drugs. Moreover, the risks and benefits of each class of these medications, including prescription, nonprescription, and alternative medicine-related products, should be judiciously considered in the case of HF.
References
- Curtis LH, Whellan DJ, Hammill BG, et al. Incidence and prevalence of heart failure in elderly persons, 1994–2003. Arch Intern Med. 2008;168(4):418.
- Nahin RL. Estimates of pain prevalence and severity in adults: United States, 2012. J Pain. 2015;16(8):769–780.
- Finnerup NB, Attal N, Haroutounian S, et al. Pharmacotherapy for neuropathic pain in adults: a systematic review and meta-analysis. Lancet Neurol. 2015;14(2):162–173.
- Wang ZY, Shi SY, Li SJ, et al. Efficacy and safety of duloxetine on osteoarthritis knee pain: a meta-analysis of randomized controlled trials. Pain Med. 2015;16(7):
1373–1385. - Liu M, Chen J, Huang D, Ke J, Wu W. A meta-analysis of proinflammatory cytokines in chronic heart failure. Heart Asia. 2014;6(1):130–136.
- DeToledo JC, Toledo C, DeCerce J, Ramsay RE. Changes in body weight with chronic, high-dose gabapentin therapy. Ther Drug Monit. 1997;19(4):394–396.
- Ho JM-W, Macdonald EM, Luo J, et al. Pregabalin and heart failure: a population-based study. Pharmacoepidemiol Drug Saf. 2017;26(9):1087–1092.
- Weis F, Beiras-Fernandez A, Sodian R, et al. Substantially altered expression pattern of cannabinoid receptor 2 and activated endocannabinoid system in patients with severe heart failure. J Mol Cell Cardiol. 2010;48(6):1187–1193.
- Rahman MM, Kopec JA, Anis AH, et al. Risk of cardiovascular disease in patients with osteoarthritis: a prospective longitudinal study. Arthritis Care Res (Hoboken). 2013;65(12):1951–1958.
- Majeed MH, Sherazi SAA, Bacon D, Bajwa ZH. Pharmacological treatment of pain in osteoarthritis: a descriptive review. Curr Rheumatol Rep. 2018;20(12):88.
- Arfè A, Scotti L, Varas-Lorenzo C, et al. Non-steroidal anti-inflammatory drugs and risk of heart failure in four European countries: nested case–control study. BMJ. 2016;354:i4857.
- Mahé I, Meune C, Diemer M, et al. Interaction between aspirin and ACE inhibitors in patients with heart failure. Drug Saf. 2001;24(3):167–182.
- Ahmed A. Interaction between aspirin and angiotensin-converting enzyme inhibitors: should they be used together in older adults with heart failure? J Am Geriatr Soc. 2002;50(7):1293–1296.
- Derry S, Moore RA, Rabbie R. Topical NSAIDs for chronic musculoskeletal pain in adults. Cochrane Database Syst Rev. 2012;(9):CD007400.
- Guedes V, Castro JP, Brito I. Topical capsaicin for pain in osteoarthritis: a literature review. Reumatol Clin. 2018;14(1):40–45.
- Grove EL, Abrahamsen B, Vestergaard P. Heart failure in patients treated with bisphosphonates. J Intern Med. 2013;274(4):342–350.
- Schnitzer TJ, Marks JA. A systematic review of the efficacy and general safety of antibodies to NGF in the treatment of OA of the hip or knee. Osteoarthr Cartil. 2015;23:S8–S17.
- Kaye DM, Vaddadi G, Gruskin SL, et al. Reduced myocardial nerve growth factor expression in human and experimental heart failure. Circ Res. 2000;86(7):E80–E84.
- Chua TP, Harrington D, Ponikowski P, et al. Effects of dihydrocodeine on chemosensitivity and exercise tolerance in patients with chronic heart failure. J Am Coll Cardiol. 1997;29(1):147–152.
- Majeed MH, Ali AA, Sudak DM. Psychotherapeutic interventions for chronic pain: evidence, rationale, and advantages. Int J Psychiatry Med. 2018:009121741879144.
- Majeed MH, Sudak DM. Cognitive behavioral therapy for chronic pain-one therapeutic approach for the opioid epidemic. J Psychiatr Pract. 2017;23(6):409–414.
- Majeed MH, Ali AA, Sudak DM. Mindfulness-based interventions for chronic pain: evidence and applications. Asian J Psychiatr. 2018;32:79–83.